

Honoring a Shared Milestone: Guyana and Barbados Mark 60 Years of Independence
By Dr. Odessa Lacsina, Executive Director, The State of Women Institute
Last month, I had the privilege of attending a special celebration marking a milestone that is both historical and personal: the 60th anniversary of independence for Guyana and Barbados, two Caribbean nations that both achieved independence in 1966, and whose enduring friendship was reflected throughout the evening.

The event, observed May 2, carried particular weight for me. As someone of both Guyanese and Barbadian heritage, I have always understood these two nations as more than geography. They are part of my story, my family's story, and the larger story of a region that has contributed so much to the world while asking for so little in return. Watching them celebrate this milestone together — with genuine warmth, shared pride, and a clear eye toward the future — filled me with a sense of gratitude I am still carrying.
The Prime Minister of Barbados traveled to Guyana for the occasion, a gesture that spoke clearly to the depth of the relationship between the two nations. Among the announcements made during the visit was a new travel arrangement designed to make it easier for citizens of Guyana and Barbados to move between the two countries — a practical expression of regional cooperation that will deepen connections between families, businesses, and communities across both nations.

L to R: Dr. Odessa Lacsina and Ishara Lacsina celebrate at the Guyana embassy; Dr. Lacsina with Sam Hinds, Guyana’s ambassador to the United States; Ishara Lacsina joins the festivities at the Embassy of Guyana.
I attended events at both embassies during the celebration. At the Embassy of Barbados, my daughter Ishara interviewed His Excellency Ambassador Victor Fernandes and met his wife, Ferida — a conversation she approached with thoughtful preparation and genuine curiosity. She also volunteered at the Guyana Embassy, welcoming guests as they arrived. Watching her engage so meaningfully with the occasion was a source of great pride. At the Embassy of Guyana, I was joined by my mother, Celeste, and had the opportunity to meet with His Excellency Ambassador Sam Hinds. To share this milestone with three generations of my family present — my mother, myself, and my daughter — made the experience especially meaningful and remains one of my most cherished memories of the celebration.

That evening, the celebrations continued with the Caribbean Film Festival, hosted jointly by the Embassies of Guyana and Barbados. The festival brought together filmmakers, artists, and storytellers whose work reflects the richness and diversity of our region — and served as a vivid reminder that Caribbean culture has always been one of our greatest forms of diplomacy, connection, and joy.
From the commemorations of independence to the celebration of Caribbean cinema, what I kept returning to was something simple: our greatest strength has always been our people. Their resilience. Their creativity. Their commitment to building stronger, healthier communities for the generations that follow.
It’s a value The State of Women Institute holds at its core — and one that was alive in every room I walked into that evening.
As Guyana and Barbados mark 60 years of independence, I am reminded that milestones like these are not only opportunities to honor the past, but also to celebrate the relationships, values, and shared aspirations that continue to shape our future. I left that evening feeling inspired by the strength of our Caribbean community and hopeful for what lies ahead. To everyone who helped make these celebrations possible, and to the generations whose sacrifices and vision brought us to this moment, I offer my deepest appreciation. May the friendship between Guyana and Barbados continue to flourish, and may both nations enjoy many more years of progress, partnership, and pride.
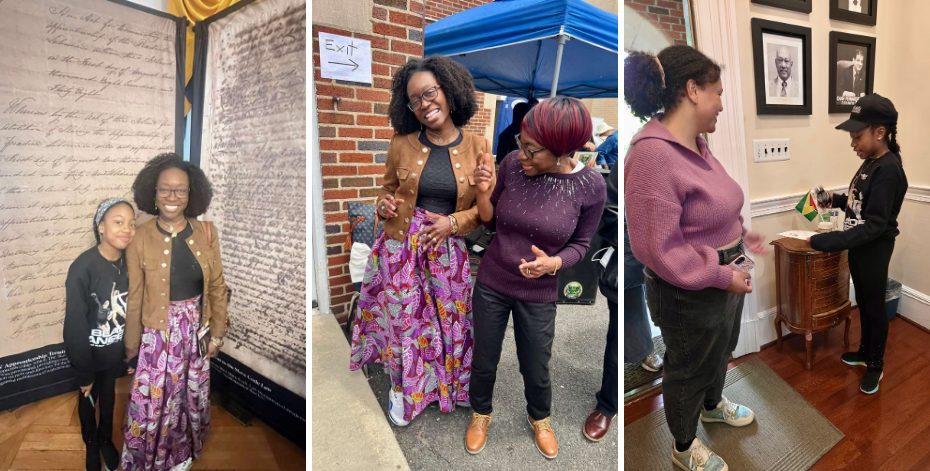
L to R: Ishara Lacsina and Executive Director Dr. Odessa Lacsina in the Embassy of Barbados; Dr. Lacsina shares a moment with her mother Celeste while celebrating at the Guyana embassy; Ishara volunteers at the Guyana embassy, greeting visitors.
Counting What Matters: Women Leading Health Equity in Guyana

The work of health equity is often described in terms of systems, policies, and outcomes. But in Guyana, I was reminded that it is first and foremost about people – and women, in particular – who carry the weight of those systems while quietly reshaping them.
By Dr. Odessa Lacsina, Executive Director, The State of Women Institute
I arrived in Guyana's capital of Georgetown just as International Women's Day was being celebrated around the world. The timing felt symbolic, but what unfolded over the following days offered an instructive view of how women lead — not in ideal conditions, but within the real constraints of geography, resources, and history. I traveled as a health equity advocate, hoping to better understand how women navigate these constraints. What I found, consistently, were resilient women leaders taking action to build systems of care where gaps still exist, and doing so with clear focus on what their communities need most.
Leadership at Every Level
My meeting with Guyana's First Lady, Arya Ali, took place on a Friday evening during a Ramadan festival near Georgetown's historic sea walls. I brought my daughter with me, wanting her to witness the importance of cultural respect and global connection. As the First Lady and I spoke about women's health, policy, and prevention, one idea she shared stood out:
“Health doesn’t wait for perfect systems. Our women can’t wait for perfect systems either — they are creating solutions now.”

L to R: Dr. Odessa Lacina at the First Lady of Guyana (Her Excellency Arya Ali ) International Women’s Day March: Empowering and celebrating women everywhere. / Hon. Minister Vindhya Persaud with Ishara Lacsina at WeLife6 Expo, an entrepreneurship conference for women and girls. Minister Persaud is responsible for policy health equity government infrastructure and economic empowerment for women. / Ishara and Dr. Odessa Lacsina with Hon. Kwame W.E. McCoy, the Minister within the Office of the Prime Minister in Guyana.
That theme surfaced again and again throughout the trip. It was present in conversations with Ministry of Health officials designing preventive care strategies, and in discussions with women leading community-based initiatives. Across these settings, there was a consistent understanding: progress depends not only on formal systems, but on the women who navigate and strengthen them every day.
Where Policy Meets Practice
In meetings with the Ministry of Health, I saw what effective policy looks like when it is informed by lived experience and led by women focused on designing health interventions that account for the realities of distance, access, culture, and daily life. This kind of leadership is often overlooked because it does not always fit neatly into traditional measures of impact. Yet it is precisely this integration of clinical knowledge with community understanding that makes health systems more responsive and durable.
These partnerships also reflect the approach that guides our work at The State of Women Institute. Health challenges do not exist in isolation, and solutions cannot either. They must reflect the full context of women's lives.
The Wisdom of Communities
The clearest lessons came during my visits to community health sites. In one community, I met a woman who had lost her sister to preventable complications during childbirth. She now leads maternal health education efforts in her region, ensuring that other families have access to information and care that her own family did not. In another, a grandmother described how she teaches traditional healing practices while encouraging younger women to seek preventive health services. Her approach was not about choosing between health systems, but about bridging them.
These are not isolated stories. They reflect a broader pattern: women translating personal experience into collective action. Their leadership operates across multiple levels — within families, across communities, and alongside formal health institutions. This is how health systems evolve in practice — beyond policy directives and through the daily work of people who understand both the gaps and the possibilities.

Left: L-R: Martina McDonald-Johnson, Managing Director, Integrated Marketing Communications; Isahra Lacsina; Dr. Alista Bishop, finance executive and author of the recently published “The Journey of Alista Bishop,” McDonald-Johnson’s daughter. Middle: Dr. Odessa Lacsina with Hon. Oneidge Walrond, Minister of Home Affairs. Right: Dr. Odessa and Ishara Lacsina as guests at the 6th Annual Guyana Women & Girls Summit.
Shared Health Challenges: Local and Global
Traveling during International Women's Day underscored something that extends beyond any one country. The barriers women face in accessing care — whether shaped by distance, cost, or system navigation — are not unique. The conversations I had in Guyana about cervical cancer prevention, maternal health, and access to health screening echoed concerns I have heard in cities across the United States. The contexts differ, but the underlying challenge is the same: how to ensure that prevention, early detection, and care are truly accessible.
It is the specificity of local solutions that allows us to see connections between different health settings and to build strategies that are both locally grounded and globally informed. Meaningful progress depends on true partnership. The leaders I met in Guyana are not waiting for external solutions — they are already advancing them. What they seek are partners who will listen, support, and help extend the reach of what is already working. Their leadership makes clear what is required next: investment, infrastructure, and sustained partnership.
This is the role The State of Women Institute is committed to playing.

Participants join First Lady Arya Ali, Minister of Human Services and Social Security Dr. Vindhya Persaud, and other Cabinet members for a vibrant walk through Georgetown in celebration of International Women’s Day. The event, which began at the Bank of Guyana and concluded at the Kingston Seawall Esplanade, symbolized unity, empowerment, and collective commitment to advancing the rights and wellbeing of women across Guyana.
Photo courtesy of the Ministry of Human Services and Social Security.
Our partnership with Guyanese health leaders will focus on amplifying existing efforts while contributing resources, platforms, and connections. The Healing Roots initiative will incorporate insights from culturally responsive prevention strategies. Our podcast network will create space for Guyanese leaders in women's health to share their work with global audiences. Our research translation efforts will highlight community-based models that can inform broader approaches to care in similar settings. The State of Women Institute's goal is to shine a spotlight where health innovation already exists — and to ensure it is supported and sustained.
Moving Health Equity Forward
As I departed Guyana, I reflected on the determined, transformative work I had witnessed. There was no sense of pause. The same women I had met would return the next day to their responsibilities — coordinating care, educating families, shaping programs, and advocating for improvements. Their efforts are already transforming health outcomes in ways that may not always be visible at scale, but are deeply felt within their communities.
The lesson from Guyana for International Women's Day is straightforward: when women lead, health systems become more responsive. When their leadership is supported, those systems become stronger. And when their insights are shared across contexts, the impact extends far beyond any single setting.
This is the kind of progress The State of Women Institute champions — not only on International Women's Day and during Women’s History Month, but on every day that follows.
Dr. Odessa Lacsina is the Executive Director of The State of Women Institute, a 501(c)(3) nonprofit working across three health equity pillars: Mental Health & Wellness, Maternal Health Equity, and Preventive Wellness. The State of Women Institute's work spans from Baltimore to international partnerships, always centered on amplifying women's voices and building the infrastructure to support community-led health solutions.
To learn more or support women's health leadership globally, visit thestateofwomen.org or follow @thestateofwomen.

Unequal Pay, Unequal Health: The Hidden Health Costs of the Pay Gap
Equal Pay Day was yesterday. The date is a calculation, but the consequences are daily: smaller paychecks shape choices that affect women’s mental health and family life. This piece explains how the numbers translate into stress, what the evidence shows about income and mental health, and which policy changes have the clearest support.
When Equal Pay Day arrives, the story is often a single statistic and a single headline. The calculation is simple: how far into the new year women must work to earn what men earned the year before. The date landed yesterday. The underlying figures did not change overnight. According to the U.S. Census Bureau, the female‑to‑male earnings ratio for full‑time, year‑round workers was 80.9 percent in 2024. The Bureau of Labor Statistics reports median weekly earnings in the fourth quarter of 2024 were $1,083 for women and $1,302 for men. Analysts at the Institute for Women’s Policy Research and the Economic Policy Institute show the gap is larger for Black and Latina women and that controlled measures widened again in 2025.
Those numbers matter in small, practical ways. A few hundred dollars a month can determine whether a family keeps a childcare slot, fills a prescription, or pays for a therapy visit. The American Psychological Association’s Stress in America surveys place money and the economy among the top stressors for adults, and women report higher levels of money‑related strain. Over time, the choices people make to stretch a paycheck accumulate into chronic stress that affects sleep, concentration, and mood.
When extra income changes health
Researchers have asked whether income itself moves mental‑health outcomes. A 2023 systematic review in PLOS One examined randomized and quasi‑experimental cash‑transfer programs and found modest but consistent reductions in depression and anxiety, with larger effects for unconditional payments. Those studies suggest that when money reaches households in need, mental‑health symptoms can fall while the support continues.
Evidence from high‑income settings is more mixed, and that matters for policy design. A 2024 study in JAMA Network Open that analyzed state minimum‑wage changes and children’s mental health found no clear, consistent improvements across a broad set of outcomes. The JAMA analysis shows that the size, duration, and targeting of income changes determine whether health outcomes shift. Small or temporary increases rarely produce the same effects as sustained, well‑targeted supports.
From these findings two practical points follow. Income can be a lever for mental‑health improvement when it reaches the households that need it. Policy must be designed to reach those households consistently and at sufficient scale.
The unpaid work that deepens the squeeze
Earnings are only half the picture. Time‑use data from the Bureau of Labor Statistics and reporting from the Pew Research Center show women still shoulder more childcare, eldercare, and household tasks. The National Partnership for Women & Families estimates unpaid care in the United States is worth more than $1 trillion annually, and women perform roughly two‑thirds of that labor.
That unpaid work pushes many women into part‑time or lower‑benefit jobs. Those positions often lack employer mental‑health coverage and paid leave. Recent analyses from 2023 to 2025 document higher rates of burnout among working mothers and a greater likelihood of leaving paid work because of caregiving demands. Over a career, interrupted earnings and missed promotions compound into large lifetime losses. The National Women’s Law Center reports that the median annual earnings gap in 2024 translated to roughly $13,570 less per year for a woman working full time compared with a man, and lifetime losses can exceed half a million dollars over a 40‑year career, with larger shortfalls for women of color.
A small sensory detail can make the arithmetic feel immediate: in a clinic waiting room, the faint smell of coffee and the rustle of a folded prescription receipt in a trash can can stand for the choice between medicine and groceries. That scrap is a quiet record of tradeoffs that accumulate into chronic stress.
How families feel the impact
Lower earnings change household choices in concrete ways. Analyses from the National Women’s Law Center and other groups show that wage gaps reduce spending on essentials such as healthcare, childcare, and nutritious food. The Kaiser Family Foundation’s surveys on women’s health document gaps in affordability and access for mental‑health services. When families delay preventive care or skip therapy because of cost, conditions that could have been managed early become harder to treat.
Public‑health literature links parental financial strain to children’s emotional and behavioral outcomes. Children raised in households with chronic economic stress show higher rates of anxiety and behavioral challenges, and those effects can persist into adolescence and adulthood. The cumulative pattern is both economic and psychological: decades of smaller paychecks, interrupted careers, and deferred care shape how households plan, how parents divide labor, and how children experience stability.
What fair pay would change, practically
If pay were fairer tomorrow, the effects would be practical and measurable.
More reliable access to care. Evidence from cash‑transfer studies shows reductions in depression and anxiety when households receive sustained income boosts. Even modest, reliable increases in income can make therapy, medications, and preventive visits affordable rather than optional.
Fewer tradeoffs between work and care. Fairer wages reduce the pressure to choose between childcare and a paycheck or between groceries and a prescription. That reduces decision fatigue and the chronic stress that contributes to burnout.
Caregiving becomes more manageable. With higher earnings, families can afford childcare, eldercare, or a few hours of paid help. That breathing room changes the rhythm of daily life and reduces emotional exhaustion.
Children grow up in calmer homes. Reduced parental stress improves children’s emotional stability, school attendance, and long‑term outcomes.
Communities gain. Higher earnings for women strengthen local economies, stabilize housing, and increase demand for services that support family health.
These outcomes depend on policy design. The JAMA Network Open study on minimum wages shows that raising wages alone does not guarantee mental‑health improvements for children. Policies that combine pay equity with caregiving supports—paid family leave, affordable childcare, pay transparency, and targeted income supports—are more likely to reach the households that need them.
Policy levers with evidence
Several policy tools have empirical support and practical logic.
Pay transparency and audits. Requiring employers to disclose pay ranges and conduct equity audits helps workers identify and correct unexplained wage differences.
Paid family leave and childcare subsidies. These reduce career interruptions that drive lifetime earnings losses and give families predictable options for care.
Targeted income supports. Refundable tax credits and child allowances lift household incomes directly and have shown mental‑health benefits in multiple studies.
Stronger enforcement of equal‑pay laws. Better enforcement can correct systemic disparities that accumulate over careers.
Equity must be central. The Institute for Women’s Policy Research and the Economic Policy Institute show the wage gap is largest for Black and Latina women. Policies that ignore race and caregiving status will leave the most affected groups behind.
How to keep the conversation going
Publishing the day after Equal Pay Day gives this piece a different shape. The date is a prompt. The work that follows is sustained. Yesterday’s headlines remind readers that the calculation exists. Today’s reporting should push beyond the ritual and into the evidence: how pay affects mental health, which policies have shown results, and which communities face the deepest losses.
Track a few indicators. Watch median earnings by gender and race. Watch mental‑health surveys that break out results by caregiving status and income. Watch evaluations of policy pilots—paid leave programs, childcare subsidies, and targeted cash supports—that measure mental‑health outcomes. Those indicators will show whether the conversation moves from a single day to lasting change.
Journalists and advocates can help by telling the stories behind the numbers. Profiles of families who face the tradeoffs between care and work make the stakes tangible. Reporting that connects wage policy to mental‑health outcomes will broaden the conversation beyond paychecks and into the daily lives of women and children.
‘Really? We Won?’ — What Nobel Laureate Claudia Goldin Means When She Says Women Won
Every time Claudia Goldin reveals the title of her ongoing research to a woman, she gets the same response. The work is called "Why Women Won," and almost without exception, the answer comes back: Really? We won?
It's a fair reaction. Open a newspaper. Look at the state of maternal mortality in the United States, the only wealthy country where it has been rising. Think about paid parental leave, which the U.S. remains nearly alone among developed nations in not guaranteeing. Think about the cost of childcare. Think about the gender pay gap that refuses to close.
And still, she means it.
March 4, just days before International Women's Day, Goldin delivered "Why Women Won" as the NIH Director's Lecture at the National Institutes of Health, one of American science's most prestigious platforms. The full talk is available to watch on the NIH videocast platform. It is an hour well spent. Goldin is the Henry Lee Professor of Economics at Harvard University and the 2023 Nobel laureate in economics, the first woman ever to win that prize unshared. This month, the American Academy of Arts and Sciences named her the recipient of its 2026 Talcott Parsons Prize, awarded every few years for high-impact contributions across the social sciences.
What she has built over a career at Harvard is harder to summarize than a list of honors. It is something closer to an archive of the economic lives of American women across two centuries, assembled from sources that other researchers either overlooked or never thought to look for.
The Economist as Detective
Goldin has described herself, since childhood, as wanting to be a detective. The Nobel committee took her at her word: her official Nobel portrait depicts her with a magnifying glass, a Sherlock Holmes hat, and a Golden Retriever. She grew up in the Bronx, attended the Bronx High School of Science intending to study bacteriology, and was redirected entirely by an economics professor at Cornell who revealed that discovery was the whole point — that economics, done right, was another form of hunting for hidden truths.
She earned her doctorate at the University of Chicago, was denied tenure at Princeton (economic history, she has noted, wasn't valued there at the time), and arrived at Harvard in 1990. Her method is to read the present through the past. In 1981, she went to the National Archives and, with a researcher's permission, rifled through boxes of Women's Bureau surveys that had sat largely untouched for decades — work histories, marriage bar records, wage data. She found surveys from 1939 in which managers, before any anti-discrimination legislation existed, answered candidly whether their firms fired women when they married. Many did. "The forms tell stories, and I listen," she has written in her Nobel biographical essay, "The Economist as Detective."
Her books include Understanding the Gender Gap: An Economic History of American Women (1990) and Career & Family: Women's Century-Long Journey Toward Equity (2021), the latter translated into fifteen languages. In announcing her as this year's Parsons Prize honoree, the Academy highlighted her pioneering work on women as economic operators — women as people who make decisions, build careers, navigate markets, and control, or don't control, their own money, their own names, their own futures.
A World Not So Long Ago
"Why Women Won" opens with a reminder that should not need to be a reminder.
Within living memory, women were routinely and legally fired when they married or became pregnant. They could not always get a credit card in their own name, or legally choose their own name. Decades after winning the right to vote, women had not yet obtained equal legal rights in the workplace, in marriage, in family law, in Social Security, in criminal justice, or in credit markets. The word "discrimination," as applied to women's treatment at work, was barely in common use — because the concept was not yet widely recognized as applicable to women at all.
Goldin has compiled a chronology of 155 critical moments in U.S. women's rights history, spanning 1908 to 2023, sorted into four categories: workplace rights, economic and social rights, political rights, and rights over their own bodies. Of those 155 moments, 45 percent occurred in a single decade, between 1963 and 1973. The Equal Pay Act. Title VII of the Civil Rights Act, with the word "sex" added almost accidentally by a congressman who initially intended it as a kill shot against the entire bill. Title IX. The Equal Credit Opportunity Act. No-fault divorce laws spreading across the states. And in January 1973, Roe v. Wade — which Goldin describes in her research as a success none of its supporters had predicted, an unexpected gift to the women's movement.
The word "fortuitous" appears more than once in her analysis of this period, and she means it precisely. The Civil Rights and anti-war movements changed everything. Women saw that their issues were not being discussed, and they learned to organize and leverage their power as an increasingly important voting bloc. But the legislative cascade that followed was not inevitable. It was contingent, fought-for, and at several critical moments, lucky.
"I find it impossible to imagine my world would be the same had women's rights remained as they were when I entered this institution as an undergraduate," Goldin told the Cornell Daily Sun. She received her undergraduate degree from Cornell in 1967, in the years just before that cascade began.
The Pill, the Paycheck, and the Body
Among Goldin's most celebrated findings is the research she conducted with Harvard colleague and husband Lawrence Katz on oral contraceptives and women's economic outcomes. The pill was approved by the FDA in 1960, initially for married women only. State laws restricting access for unmarried women were common. In her Nobel biographical essay, Goldin described the reality for young women of her own Cornell generation: putting fake rings on their fingers to convince doctors they were married, in order to get a prescription.
The state laws changed at different times and in ways that were effectively random, and Goldin and Katz used that variation as a natural experiment to measure the pill's causal effect on women's professional lives. Access to the pill increased the age at which women first married, which meant women could invest more heavily in professional training before family obligations arrived. Women made up 10 percent of first-year law students in 1970. By 1980, they made up 36 percent — a shift that coincided almost exactly with the cohort that came of age with access to contraception. Women with access to the pill experienced narrower wage gaps than those without.
Goldin's own chronology of women's rights, which runs through 2023, names Dobbs v. Jackson Women's Health Organization — the 2022 Supreme Court decision that overruled Roe v. Wade — explicitly among the history's documented "downs."
Why the Gap Persists
Legal rights, even sweeping ones, did not close the gender pay gap. In her American Economic Association presidential address, Goldin argued that the primary driver of the remaining gap was not discrimination in the traditional sense. It was the structure of work itself.
She describes certain positions as "greedy jobs" — those that disproportionately reward long hours, constant availability, and relentless schedule flexibility. These jobs pay substantially more than positions with predictable hours. And because women continue to carry a disproportionate share of caregiving at home, they disproportionately step back from these positions when family obligations arrive. The pay gap that results is not mainly employers paying women less for identical work. It is couples making rational choices inside a system that penalizes the person who takes the 3 p.m. call from school.
Why Women Are Divided
"Why Women Won" does not stop at the victories. It takes on the harder question in Goldin's research: why are women so divided about the very rights that would benefit them?
Her answer, drawn from decades of polling data including Gallup surveys, the General Social Survey, and the American National Election Studies, is that divisions among women by marital status, employment, religion, and region have consistently been greater than the divisions between men and women as a whole. This was true before the women's movement peaked in the early 1970s, and it deepened as the movement succeeded. Each legislative win caused some women to feel their goals were met and step back from organizing, leaving the remaining voices to appear increasingly radical to outsiders. The traditionalist and anti-feminist movement that organized in the early 1970s — initially around opposition to the ERA, then galvanized further by Roe v. Wade — remains, as Goldin writes in her NBER paper, a potent force in American politics today.
The word "feminist" became a casualty along the way. Even when large majorities of Americans supported expanding women's rights, Goldin's polling data shows that almost no one in any era would apply that word to themselves. The demonization of the term was not accidental. It was one of the most effective tools the opposition had, and its impact is still measurable in the data.
Rights Without Infrastructure
The comparison with peer nations sits near the center of Goldin's argument. The United States led other wealthy countries in granting women formal legal rights. It has lagged most of them, significantly, in providing the practical support that makes those rights livable. The U.S. led in terms of codifying rights but continues to lag in support for maternity and parental leave and childcare, compared to other industrialized countries.
American women won access to law school, medical school, credit, and equal employment protection. What they did not win — what women in Germany, Sweden, Canada, and Japan gained alongside or in place of formal legal equality — was the infrastructure: paid leave, subsidized childcare, labor structures that don't demand a binary choice between professional ambition and having a family. Goldin's research suggests this was not simply a political failure of timing. The traditionalist movement specifically and effectively stymied progress on paid family leave and subsidized childcare. Those consequences are still being lived.
The Long View
When asked whether she is pessimistic about the future of women, Goldin points to the smiley face she puts beside the word "won" in her talk title. "People often ask me if I'm pessimistic about the future of women," she has said. "Which is why I put that happy face on."
The optimism is archival, not sentimental. Goldin has spent her career with the actual data of actual women's lives across more than a century, assembled document by document from archives and survey boxes and old city directories. From that vantage point, what the record shows is plain: things were worse before. Specifically, documentably, legally worse. Not so long ago.
The history she has built includes Dobbs. It includes the defeat of the Equal Rights Amendment. It includes organized opposition that stalled paid family leave for a generation. The arc she traces is not smooth. It is a record of what was won, by whom, through what combination of strategy and luck and sustained pressure, and what it cost when parts of it slipped back.
That is, finally, the point of the title. Not a declaration that the work is done. A documented account of how much has already been accomplished — and a foundation from which the next chapter can be written with some knowledge of what the earlier ones actually contained.
Dr. Claudia Goldin's research, including the NBER working paper "Why Women Won," is publicly available at nber.org. Her book Career & Family: Women's Century-Long Journey Toward Equity is available wherever books are sold. The American Academy of Arts and Sciences will formally present her with the 2026 Talcott Parsons Prize on April 16.
Photo by Editing1088, licensed under CC BY-SA 4.0. Source: https://creativecommons.org/licenses/by-sa/4.0/
Sources
"Why Women Won" — NIH Director's Lecture, March 4, 2026. Event page and full videocasthttps://oir.nih.gov/wals/2025-2026/why-women-won
"Why Women Won" — NIH Videocast (full lecture, free to watch)https://videocast.nih.gov/watch/924bddcc-0174-11f1-9f14-124f0a52e769
"Why Women Won" — NBER Working Paper No. 31762, Claudia Goldin (October 2023, revised September 2025)https://www.nber.org/papers/w31762
"Claudia Goldin Wins Talcott Parsons Prize for Social Scientists" — Harvard Gazette, March 5, 2026https://news.harvard.edu/gazette/story/newsplus/claudia-goldin-wins-talcott-parsons-prize-for-social-scientists/
"The Economist as Detective" — Claudia Goldin Nobel Biographical Essay, NobelPrize.orghttps://www.nobelprize.org/prizes/economic-sciences/2023/goldin/biographical/
Career & Family: Women's Century-Long Journey Toward Equity — Claudia Goldin, Princeton University Press (2021)https://press.princeton.edu/books/hardcover/9780691201788/career-and-family
Understanding the Gender Gap: An Economic History of American Women — Claudia Goldin, Oxford University Press (1990)https://global.oup.com/academic/product/understanding-the-gender-gap-9780195072709
"The Power of the Pill: Oral Contraceptives and Women's Career and Marriage Decisions" — Claudia Goldin and Lawrence F. Katz, Journal of Political Economy (2002)https://www.journals.uchicago.edu/doi/10.1086/340778
Claudia Goldin — full publications list, Harvard Universityhttps://scholar.harvard.edu/goldin/publications
Patient Recognition Week: Why Women Deserve to Be Believed the First Time
What does it mean to truly recognize a woman as a patient? It means believing her pain the first time she describes it, and treating her as the expert on her own body. During National Patient Recognition Week, that shift—from doubting to trusting, from brushing off to leaning in—may be one of the most powerful ways healthcare can honor women’s lives.
Checking in on Patients
National Patient Recognition Week, observed February 1–7, was created to spotlight patient satisfaction, empathy, and human-centered care in clinics and hospitals across the United States. Healthcare organizations are encouraged to listen more carefully, encourage feedback, and recommit to compassionate treatment and respect for every person who walks through their doors.
In 2026, the theme emphasizes hearing and respecting patients’ voices and weaving their lived experience into care decisions. Some organizations mark the week with social media campaigns, appreciation notes, or small events; others use it to review communication practices and experience surveys with an eye toward real improvement. The week strives to ask a basic question: Do patients feel like human beings whose stories matter, not just the next name on a schedule?
For many women, the honest answer is still “not always.”
When Women’s Pain Isn’t Believed
Decades of research show that women’s pain is more likely than men’s to be minimized, psychologized, or misattributed, even when symptoms are similar. Studies and clinical reviews have documented patterns where women describing pain are more often told their symptoms are due to stress or emotions, while men with comparable complaints are offered diagnostic tests or stronger pain relief. Old stereotypes about women being “dramatic” or “hysterical” may be out of fashion in name, but they linger in how some symptoms are interpreted.
The stakes are high. Chronic pain conditions that disproportionately affect women—endometriosis, pelvic pain, interstitial cystitis, vulvodynia, certain autoimmune conditions—can take years to diagnose. In that time, a woman may see multiple providers, repeat her stories over and over, and still feel like no one appreciates the intensity of her symptoms, reality of her experience, or depth of her concerns. When a clinician finally listens and takes their words seriously, it can change the course of a patient’s care: Treatment plans are adjusted, imaging ordered, referrals made, and women stop hearing that it’s “all in your head.”
Here, “recognition” isn’t a slogan or a card on a bulletin board. It’s what happens when a provider hears a woman describe her pain and automatically treats that account as credible and important. It starts with belief rather than skepticism.
When Women Are Missing From the Data
Bias doesn’t only show up in the exam room. It’s also baked into the research that shapes standards of care. For years, clinical trials often under-enrolled women or failed to analyze sex-specific data, treating male bodies as the norm and female bodies as a variation on that norm. Policies have improved, but major gaps remain, especially for conditions that primarily or exclusively affect women.
Pain management is one example. Reviews of the field highlight how stereotypes, unequal study designs, and a lack of high-quality, gender-aware research all feed into misdiagnosis and undertreatment of women’s pain. When diseases, devices, and drugs are studied in populations that don’t reflect women’s bodies and lives, the message is clear: women’s health isn’t driving the agenda.
If Patient Recognition Week is about honoring the patient voice, then for women that has to include research that reflects their realities. Recognition isn’t only “We’ll listen during your appointment.” It also means, “We’re designing studies, treatments, and protocols with you in mind.”
Heart Disease: The Risk Women Don’t Expect
Heart disease shows how belief and representation in the data both matter. Cardiovascular disease is the leading cause of death in women worldwide and in the United States, responsible for an estimated 30% of deaths among women—more than all forms of cancer combined. Yet many women still don’t recognize heart disease as their top health threat, and gender bias has contributed to under-diagnosis and under-treatment.
Symptoms can look different in women. Instead of the classic “crushing chest pain” image that’s often associated with men, women may experience severe fatigue, shortness of breath, nausea, lightheadedness, or pain in the back, jaw, or neck. Those complaints are easy to dismiss as anxiety, indigestion, or stress—by women themselves and sometimes by their providers. Time is lost, and so is trust.
Patient recognition here means clinicians are trained to look for sex-specific patterns, take these symptoms seriously, and treat a woman’s sense that “something isn’t right” as a critical piece of information. Public messaging matters too: awareness campaigns that speak directly to women’s risks and symptoms help women know when to seek care.
The Hidden Cost of Asking Women to “Advocate Harder”
Women are often told to advocate for themselves in medical settings: ask more questions, bring a list, speak up if something feels off. Those tools can help, and practical strategies like symptom logs, written questions, or bringing a friend do make it easier to get clear answers. But when the system doesn’t change, “self-advocacy” can quietly shift responsibility onto women for fixing the bias they face.
Experts in women’s health and pain management note that many women brace for their symptoms to be doubted, especially when they involve reproductive health, pelvic pain, or conditions that mainly affect women. That constant vigilance comes at a cost. It’s draining to walk into every appointment assuming you’ll have to prove your own pain. It’s wearing to tell the same story again and again, hoping that this time someone will take it seriously.
Patient Recognition Week gives clinics and health systems a chance to turn away from that pattern. Instead of asking women to fight harder, they can ask what it would look like to listen better and change structures that make women feel unheard in the first place.
What True Recognition Could Look Like
If healthcare decided to use this week to genuinely recognize women as experts in their own bodies, a few practical steps could make a real difference.
Listening sessions with women patients. Clinics can host small listening circles or online surveys inviting women from different backgrounds to share moments when they felt heard—and when they didn’t. Themes from those conversations can inform staff training, appointment workflows, and communication policies.
Gender-aware training on pain and symptoms. Ongoing education can help providers spot the ways gender bias creeps into pain management and diagnosis, from assuming women exaggerate symptoms to overlooking heart disease when complaints don’t fit the “classic” pattern. Small adjustments—a different follow-up question, a lower threshold for testing—can prevent years of missed or delayed care.
Clear protocols for women’s health conditions. Building or updating clinical pathways for endometriosis, chronic pelvic pain, and other women’s health issues signals that the clinic expects these conditions, takes them seriously, and has a plan. That can make women feel less like outliers and more like patients whose needs were anticipated.
Better feedback loops. Instead of relying only on generic satisfaction surveys, organizations can ask women specific questions: “Did you feel listened to?” “Did your provider believe your description of your symptoms?” “Did you feel safe talking about pain or sensitive concerns?” Responses can drive concrete changes in scheduling, staffing, or communication tools.
Centering women in public messaging. During heart health campaigns in February or Patient Recognition Week posts, including women-focused risk information and symptom lists makes messages more accurate and more useful. When women see their experiences described, they’re more likely to recognize warning signs and seek care.
None of this replaces the need for skilled clinicians, strong science, or evidence-based treatments. Medical expertise and high-quality research are essential foundations. The point is to pair that expertise with the knowledge women have about their own bodies and lives, rather than treating those experiences as secondary.
For Women Reading This: You Deserve to Be Believed
If you’re a woman who’s been told “it’s probably nothing” when it didn’t feel that way, you’re not alone. If you’ve had a provider wave off your pain or walked out of an appointment thinking, “They didn’t really hear me,” that experience is unfortunately common—and it’s part of a larger pattern, not a personal shortcoming.
A few simple steps can make medical visits feel more manageable:
Write down the basics ahead of time. Note your main symptoms, when they started, what makes them better or worse, and what you’re most worried about. You don’t need medical language; your own words are enough.
Bring someone you trust. A friend or family member can help you remember details, take notes, or speak up if you get flustered.
Keep one or two key questions in mind. Questions like “What else could this be?” or “If I were your sister, what would you recommend next?” can open the door to clearer explanations and more thoughtful care.
These strategies can’t fix systemic bias on their own, and they shouldn’t have to. But they can give you a bit more steadiness in the room while broader changes take shape.
A Week to Ask Better Questions
National Patient Recognition Week often shows up in warm social media posts and cheerful graphics celebrating patients—and that kindness matters. It’s also a natural point in the calendar for clinics and health systems to ask harder questions: Do women feel believed here? Do they feel their pain counts? Do they see themselves reflected in our research, our protocols, and our public messaging?
Recognizing women as patients means treating them as central decision-makers and credible narrators of their own health, not passive recipients of care. It means acknowledging the research gaps and diagnostic patterns that have left women under-diagnosed and under-treated, and then doing something about them. It means understanding that the best care comes from combining medical knowledge with the lived experience women bring into the exam room.
If you work in healthcare, this week is a chance to talk with women in your practice, examine where bias might be showing up, and pick at least one concrete change that makes it easier for women to be believed the first time they speak. If you’re a patient, it’s a reminder that your symptoms are real, your perspective matters, and you have every right to care that treats you as the expert on your own body.
That’s the kind of recognition women’s health has been missing—and the kind that can spare years of suffering, and sometimes, save lives.
Sources
“The Girl Who Cried Pain: A Bias Against Women in the Treatment of Pain”
https://pubmed.ncbi.nlm.nih.gov/11521267/
American Medical Women's Association - Pain Management Review
https://amwa-doc.org/pain-management-reviewing-research-that-highlights-differences-in-pain-assessment-and-management-between-patients/
Cardiometabolic Health Alliance - Heart Disease as #1 Cause of Death for Women
https://www.cardiometabolichealth.org/heart-disease-remains-leading-cause-of-death-for-women-addressing-the-gender-bias-in-cardiovascular-care/
World Heart Federation - Women & CVD
https://world-heart-federation.org/what-we-do/women-cvd/
Holding Ground on Maternal Health: What Maternal Health Awareness Day Means in 2026
January 23 marks Maternal Health Awareness Day, an annual observance that confronts an uncomfortable truth: pregnancy and childbirth in the United States remain far more dangerous than they should be. For a country that spends more on healthcare per capita than any other developed nation, our maternal mortality rates tell a different story.
This year’s theme, “Holding Ground on Maternal Health,” chosen by American College of Obstetricians and Gynecologists, isn’t about celebrating motherhood or sharing feel-good statistics. It's about reckoning with the preventable deaths, the widening disparities, and the systemic failures that make bringing life into the world a matter of survival for too many women.
The Numbers Tell a Grim Story
The United States has the highest maternal mortality rate among developed nations. Maternal deaths surged dramatically from 658 in 2018 to a devastating peak of 1,205 in 2021—the highest in over 50 years. While COVID-19 played a significant role in that spike, the underlying crisis predates the pandemic.
The overall numbers have improved since 2021, dropping to 817 deaths in 2022 and 669 in 2023. But those improvements haven't been shared equally, and the racial disparities have actually worsened.
Black women face a maternal mortality rate of 50.3 deaths per 100,000 live births—more than three times higher than white women at 14.5 per 100,000. Hispanic women have a rate of 12.4 per 100,000, and Asian women 10.7 per 100,000.
What's especially troubling is that the gap has widened. In 2021 and 2022, Black women died at rates about 2.6 times higher than white women. By 2023, that disparity increased to 3.5 times higher. As the pandemic eased and overall maternal deaths declined, white and Hispanic women saw significant decreases, while rates for Black women remained essentially unchanged.
What makes these statistics even more troubling is that they're largely preventable. According to research from organizations like the CDC Foundation and March of Dimes, up to 80% of pregnancy-related deaths could be avoided with timely intervention, proper screening, and continuity of care.
The problem isn't a lack of medical knowledge. We know what causes maternal deaths. We know how to prevent them. What we're missing is the infrastructure, the prioritization, and often the will to make sure every pregnant person has access to the care they need.
Most Deaths Happen After Delivery
Here's something that surprises many people: the majority of maternal deaths don't occur during labor or delivery. They happen in the weeks and months after birth.
The postpartum period has long been treated as an afterthought in American healthcare. A single six-week check-up became the standard decades ago, and for many women, that's still all they get. But complications like blood clots, infections, uncontrolled high blood pressure, and mental health crises don't always show up on a predictable timeline.
Hemorrhage, hypertensive disorders like preeclampsia and eclampsia, cardiovascular conditions, infections, blood clots, and mental health emergencies including suicide are among the leading causes of maternal death. Many of these conditions can develop or worsen well after a woman leaves the hospital.
Despite this, insurance coverage for comprehensive postpartum care remains inconsistent. Many providers don't have systems in place to track patients after discharge or follow up when warning signs appear. Women are often left to self-monitor and self-advocate at a time when they're exhausted, overwhelmed, and adjusting to life with a newborn.
Maternity Care Deserts Are Expanding
If you live in a major city, it might be hard to imagine not having access to a hospital with a maternity ward. But for over 2 million women across the United States, that's reality. They live in counties with no hospital offering obstetric care, no birth center, and no OB-GYN.
Rural communities have been hit hardest. Since 2022, more than 100 hospitals across the United States have closed their obstetric units. Maternity wards across the South and Midwest have shuttered at alarming rates over the past decade, driven by financial pressures, staffing shortages, and consolidation of healthcare systems.
The economics are brutal: maternity units must operate 24/7, but reimbursement rates don't cover costs, especially for smaller community hospitals. Women are traveling hours to deliver their babies, sometimes delivering in emergency rooms that aren't equipped for childbirth.
The Maternal Health Workforce Crisis
The maternal health workforce is shrinking, and it's not just about hospital closures. Multiple factors are driving providers out of the field:
Nearly 30% of OB-GYNs report experiencing burnout, and 23% deal with both burnout and depression. Forty percent say their work-life balance has gotten worse over the past three years. The administrative burden—excessive paperwork, charting requirements, and bureaucratic tasks—compounds the stress of an already demanding specialty.
But burnout isn't the only problem. There simply aren't enough training spots to meet demand. In the 2025 Match, 2,151 applicants competed for only 1,587 OB-GYN residency positions, leaving 564 qualified applicants without a spot. Even if every position were filled, we still wouldn't have enough OB-GYNs, midwives, and labor and delivery nurses to safely staff maternity units across the country.
The shortage is most acute in underserved and rural communities, where it's harder to recruit providers. And the underlying issue goes deeper: the care of women and children has been chronically undervalued in the broader healthcare system—underfunded in reimbursement rates and overlooked in policy priorities.
This creates a dangerous gap. When care is far away or providers are stretched too thin, women miss appointments. Complications go undetected. Risk factors pile up. And when something goes wrong, there's no safety net close by.
Mental Health Is Part of Maternal Health
Postpartum depression and anxiety affect about 1 in 7 new mothers, but many cases go undiagnosed or untreated. Postpartum psychosis is rarer but can be life-threatening when it occurs.
Suicide and overdose are among the leading causes of death in the first year after giving birth. Yet mental health screening during pregnancy and the postpartum period remains inconsistent across the country. Access to treatment is even more fragmented.
There's still stigma around admitting you're struggling after having a baby. New mothers are expected to be glowing, grateful, and bonded to their infants. When reality doesn't match that picture, many women suffer in silence rather than ask for help.
Supporting maternal health means recognizing that emotional and psychological well-being are just as critical as physical recovery. Screening needs to happen routinely, not as an afterthought. Treatment needs to be accessible, affordable, and free of judgment.
How Women Are Treated Matters
One of the most well-documented factors in maternal mortality is the quality of care women receive—and specifically, whether they're listened to and believed when they raise concerns.
Study after study has shown that Black and Indigenous women report being dismissed, ignored, or disbelieved when they talk about pain or symptoms during pregnancy and after birth. This isn't anecdotal. It's measurable, it's pervasive, and it's deadly.
Even high-profile cases have highlighted this issue. Serena Williams, one of the greatest athletes in the world, had to fight to get her medical team to take her concerns seriously after giving birth, despite her history of blood clots. If someone with her resources and platform faces that kind of dismissal, what happens to women without those advantages?
Culturally competent, trauma-informed, patient-centered care isn't optional. It's essential. Women need to be treated with dignity and respect, especially when they're at their most vulnerable. Their lived experiences and knowledge of their own bodies should be valued, not questioned.
What You Can Actually Do
Maternal Health Awareness Day isn't just about raising awareness—it's about turning that awareness into action.
Advocate for policy change. Support Medicaid expansion, paid family leave, and federal and state legislation that funds maternal health programs and addresses racial disparities. The Black Maternal Health Momnibus Act represents comprehensive legislation specifically designed to tackle maternal health inequities. Contact your representatives. Make your voice heard.
Support community organizations. Many grassroots groups are filling gaps in the healthcare system by providing doula services, prenatal education, lactation support, and postpartum care—especially in underserved communities. Organizations like the National Birth Equity Collaborative, Black Mamas Matter Alliance, March of Dimes, and local community health centers often operate on limited budgets and rely on donations and volunteers.
Educate yourself and others. Share accurate information about maternal health. Challenge myths. Talk about the realities of pregnancy and postpartum recovery, not just the sanitized version that gets posted on social media. Reliable sources include the American College of Obstetricians and Gynecologists (ACOG), the CDC Foundation's Hear Her Campaign, and organizations centered on birth equity.
Amplify lived experiences. Listen to mothers, especially those from marginalized communities. Their stories reveal what data alone cannot. They show where systems fail, where support is lacking, and where change is desperately needed.
Stories Behind the Statistics
Behind every maternal mortality statistic is a person. A mother who didn't come home from the hospital. A family forever changed by a loss that should never have happened. A survivor who fought through complications that proper care could have prevented.
We need to hear from OB-GYNs who are tracking patterns in their patients and seeing firsthand where the system breaks down. From midwives expanding access in rural areas where hospitals have closed. From doulas supporting families through traumatic births. From mothers who've had to fight to be believed when they knew something was wrong.
These stories don't just humanize the crisis. They show us where change is possible and who's already doing the work to make it happen.
Holding the Ground
This Maternal Health Awareness Day, we're holding ground.
We're not backing down on the demand for equitable, accessible, respectful care for every pregnant and postpartum person in this country. We're not accepting maternal mortality rates that belong in the last century. We're not pretending that awareness alone will solve this crisis.
Mothers deserve better. Families deserve better. Communities deserve better.
And we have the knowledge, the tools, and the resources to make it happen. What we need now is the commitment to follow through.
Resources:

How Digital Violence Is Blocking Women’s Health in the Digital Age
Human Rights Day closes out the 16 Days of Activism, and this year’s theme—“UNiTE to End Digital Violence against All Women and Girls”—lands right in the middle of how women get health care today. More and more appointments, test results, birth control consults, and mental health check-ins happen through screens, apps, and portals—and digital violence is quietly pushing women away from those tools.
This isn’t just about “being safer online.” It’s about whether women and girls feel safe enough to reach for the care they need.
1. Digital violence is changing how women seek care
When a woman has been stalked, doxxed, or threatened online, opening a health portal or a telehealth app can feel risky, even if she trusts her provider. Fear that messages, photos, or location data could be leaked or weaponized can make her cancel appointments, avoid online booking systems, or stick to walk-in clinics instead of consistent care.
For survivors of digital violence, every notification can feel like a potential new attack. That kind of fear doesn’t just live in the mind; it can lead to missed screenings, delayed follow-ups, and untreated conditions because the digital doorway to care doesn’t feel safe.
2. Sexual and reproductive health care is especially vulnerable
Sexual and reproductive health information is already highly sensitive. Add digital violence, and many women start to worry that their search history, period tracking, telehealth abortion consults, or STI testing reminders could be exposed or used against them.
Partners or family members who monitor devices, demand passwords, or “check up” on messages can make it nearly impossible for women and girls to privately access contraception, abortion care, or information about consent and healthy relationships. That’s not a small inconvenience; it can change whether someone can plan a pregnancy, leave an abusive situation, or manage an infection in time.
3. The gender digital divide is also a health divide
In many places, women have less access to phones, data, and private internet—even as health systems move more services online. When a woman relies on a shared phone, a public computer, or a device controlled by a partner, she’s more exposed to digital abuse and has fewer safe ways to use digital health tools.
That means reminders, lab results, mental health chats, and contraceptive counseling may all run through channels where someone else can see or intercept them. The result is a double hit: greater risk of digital harassment and fewer safe, private options for getting care or accurate health information.
4. Privacy and data protection are now core health issues
Digital health tools collect all kinds of information: symptoms, sexual history, mental health notes, location, even details about pregnancy or abortion. When women hear stories about data breaches, tracking, or apps sharing sensitive details without clear consent, they may decide it’s safer not to use those tools at all.
That loss of trust can be its own kind of harm. Some women stop using mental health apps, delete period trackers, or avoid signing up for online portals, even when those tools could help them manage chronic conditions or stay on top of screenings. On Human Rights Day, it’s worth saying plainly: protecting women’s health data, and making sure it can’t be used to target or shame them, is part of the right to health in a digital world.
5. Digital trauma can follow women into the clinic
For women who have faced image-based abuse, online sexual harassment, or doxxing, opening a health app or logging into a telehealth visit can bring up memories of earlier violations. That “technology-related trauma” can make it hard to answer sensitive questions honestly, turn on a camera, or trust a message system—even with a kind provider on the other side.
This can be especially intense for people seeking abortion care, contraception, STI treatment, or mental health support after sexual violence. If a digital tool feels even a little unsafe or confusing, many survivors will simply drop out of care, or postpone it until things are more serious—adding to both physical and emotional strain.
6. Health workers need to see digital safety as part of care
Doctors, nurses, midwives, school health staff, and counselors are on the front lines of women’s health in this digital moment. When a woman seems hesitant about telehealth, avoids using the portal, or misses online follow-ups, it might not be “non-compliance”—it might be fear of digital surveillance, harassment, or leaks.
Simple questions like “Do you feel safe using your phone for health messages?” or “Is there anyone else who can see your health app or texts?” can open the door to better support. Providers can help women think through safer options—like using code words, turning off certain notifications, or scheduling in-person visits—so digital tools support health instead of becoming another source of harm.
7. The right to health includes safe digital spaces
Human Rights Day is about the promise that everyone has the right to the highest attainable standard of physical and mental health. In 2025, that promise has to include the right to use digital health tools—telehealth, apps, portals, messaging—without fear of violence, harassment, or misuse of deeply personal information.
Ending digital violence against women and girls isn’t only about stopping abuse on social media. It’s also about making sure women can check their lab results, message a doctor, manage a chronic condition, or access sexual and reproductive health care without wondering who might be watching or waiting to hurt them. When digital spaces are safer, women’s access to care expands, their mental and physical health improve, and the right to health becomes a little more real—on every screen, in every clinic, for every woman and girl.

16 Days of Activism: Why Digital Violence Against Women Demands Our Attention

Image: UN Women
Every ten minutes last year, a woman or girl was intentionally killed by a partner or family member. That's 137 women and girls every single day—around 50,000 over the course of 2024. These aren't abstract numbers. They're mothers, daughters, sisters, friends, colleagues—people with dreams and plans and voices that were silenced.
And increasingly, that violence starts long before physical harm occurs. It begins with a message. A threat. A stolen photo. A deepfake created by artificial intelligence. The latest UN report shows that technology-facilitated violence—like cyberstalking, coercive control, and image-based abuse—can be a risk factor that escalates offline and, in some cases, leads to femicide.
When screens become weapons
From November 25 through December 10, the world marks the 16 Days of Activism against Gender-Based Violence. This year's theme—"UNiTE to End Digital Violence against All Women and Girls"—addresses one of the fastest-growing forms of abuse women face.
What starts small on screens can quickly spiral into threats and violence in real life. Private photos get stolen and shared without consent. Lies spread within seconds. Women's locations are tracked. AI gets weaponized to create deepfakes designed to shame and silence.
The digital world should empower women and girls. Instead, for millions of them, it's become a minefield.
Who's affected most?
Digital violence targets women more than men, especially those with public or online visibility—activists, journalists, women in politics, human rights defenders, and young women. The impact hits even harder for women facing other forms of discrimination based on race, disability, gender identity, or sexual orientation.
Adolescent girls face some of the greatest risks. Their social and emotional development increasingly happens online, in spaces filled with gender bias and misogyny that can fuel lasting harm.
Consider the journalist who stops writing after death threats. The activist who deletes her accounts to protect her family. The girl who loses confidence before she's even found her voice.
Why the focus on digital violence now?
Several factors have converged to make digital violence a crisis that can't be ignored:
Weak regulation of the technology sector means there's often no legal recognition of digital violence in many countries. Tech platforms lack accountability. Misogynistic content in the so-called "manosphere" fuels abuse and spreads hate. When these toxic ideas go viral, they shape how entire generations see and treat women and girls.
AI has created new forms of abuse and amplified existing violence. There's a growing backlash against gender equality. The anonymity of perpetrators and cross-border nature of online abuse make it harder to get justice. Support systems for survivors remain limited.
And here's the thing: this is happening at a time when sweeping aid cuts are forcing women's organizations around the world to shut down or drastically scale back programs to end violence against women.
Progress and the road ahead
There's been some movement in the right direction. Thanks to years of advocacy by feminist and digital rights movements, major progress has been made. In 2024, the UN Statistical Commission called for the development of global methods to measure technology-facilitated gender-based violence. Regional bodies have acted too—from the African Union's Convention on Ending Violence against Women and Girls to the EU's Digital Services Act.
But we can't stop there.
#NoExcuse for violence
There is #NoExcuse for violence against women and girls. Nearly one in three women experience violence in their lifetime. For adolescent girls, the statistics are even more concerning: one in four is abused by their partners.
This year's 16 Days of Activism campaign has clear calls to action for different groups:
Governments need to pass and enforce laws that criminalize digital violence, protect personal information, and strengthen tech sector accountability.
Tech companies must ensure platform safety, remove harmful content quickly, enforce codes of conduct, and publish transparent reports about how they're addressing abuse.
Donors should invest in feminist organizations working to end violence against women and support digital rights advocates.
All of us can speak out, support survivors, and challenge harmful online norms. We can build critical thinking skills around online content, consent, and respectful relationships.
The bigger picture
The 16 Days of Activism runs from November 25 — the International Day for the Elimination of Violence Against Women — through December 10, which is International Human Rights Day. That connection isn't accidental.
Violence against women is a human rights issue. And as we approach the 30th anniversary of the Beijing Declaration and Platform for Action in 2025—one of the most important international agreements on women's rights—this campaign serves as a reminder that digital safety is central to gender equality.
Women belong online. Girls belong online. But they deserve to be there safely.
What comes next
Violence against women and girls can and must be prevented. This requires ending impunity by holding perpetrators accountable. It means adopting, implementing, and funding National Action Plans to end violence against women and girls. It calls for investing in prevention and women's rights organizations to ensure survivors have access to essential services.
The work isn't easy. But better to try, better to be on the right side of history, better to do the part that each of us can do.
Because there's #NoExcuse for violence. Not in person. Not online. Not anywhere.
The 16 Days of Activism against Gender-Based Violence runs from November 25 to December 10. Learn more about how to get involved at UN Women.
Follow the conversation using #NoExcuse and #16Days.