

Honoring a Shared Milestone: Guyana and Barbados Mark 60 Years of Independence
By Dr. Odessa Lacsina, Executive Director, The State of Women Institute
Last month, I had the privilege of attending a special celebration marking a milestone that is both historical and personal: the 60th anniversary of independence for Guyana and Barbados, two Caribbean nations that both achieved independence in 1966, and whose enduring friendship was reflected throughout the evening.

The event, observed May 2, carried particular weight for me. As someone of both Guyanese and Barbadian heritage, I have always understood these two nations as more than geography. They are part of my story, my family's story, and the larger story of a region that has contributed so much to the world while asking for so little in return. Watching them celebrate this milestone together — with genuine warmth, shared pride, and a clear eye toward the future — filled me with a sense of gratitude I am still carrying.
The Prime Minister of Barbados traveled to Guyana for the occasion, a gesture that spoke clearly to the depth of the relationship between the two nations. Among the announcements made during the visit was a new travel arrangement designed to make it easier for citizens of Guyana and Barbados to move between the two countries — a practical expression of regional cooperation that will deepen connections between families, businesses, and communities across both nations.

L to R: Dr. Odessa Lacsina and Ishara Lacsina celebrate at the Guyana embassy; Dr. Lacsina with Sam Hinds, Guyana’s ambassador to the United States; Ishara Lacsina joins the festivities at the Embassy of Guyana.
I attended events at both embassies during the celebration. At the Embassy of Barbados, my daughter Ishara interviewed His Excellency Ambassador Victor Fernandes and met his wife, Ferida — a conversation she approached with thoughtful preparation and genuine curiosity. She also volunteered at the Guyana Embassy, welcoming guests as they arrived. Watching her engage so meaningfully with the occasion was a source of great pride. At the Embassy of Guyana, I was joined by my mother, Celeste, and had the opportunity to meet with His Excellency Ambassador Sam Hinds. To share this milestone with three generations of my family present — my mother, myself, and my daughter — made the experience especially meaningful and remains one of my most cherished memories of the celebration.

That evening, the celebrations continued with the Caribbean Film Festival, hosted jointly by the Embassies of Guyana and Barbados. The festival brought together filmmakers, artists, and storytellers whose work reflects the richness and diversity of our region — and served as a vivid reminder that Caribbean culture has always been one of our greatest forms of diplomacy, connection, and joy.
From the commemorations of independence to the celebration of Caribbean cinema, what I kept returning to was something simple: our greatest strength has always been our people. Their resilience. Their creativity. Their commitment to building stronger, healthier communities for the generations that follow.
It’s a value The State of Women Institute holds at its core — and one that was alive in every room I walked into that evening.
As Guyana and Barbados mark 60 years of independence, I am reminded that milestones like these are not only opportunities to honor the past, but also to celebrate the relationships, values, and shared aspirations that continue to shape our future. I left that evening feeling inspired by the strength of our Caribbean community and hopeful for what lies ahead. To everyone who helped make these celebrations possible, and to the generations whose sacrifices and vision brought us to this moment, I offer my deepest appreciation. May the friendship between Guyana and Barbados continue to flourish, and may both nations enjoy many more years of progress, partnership, and pride.
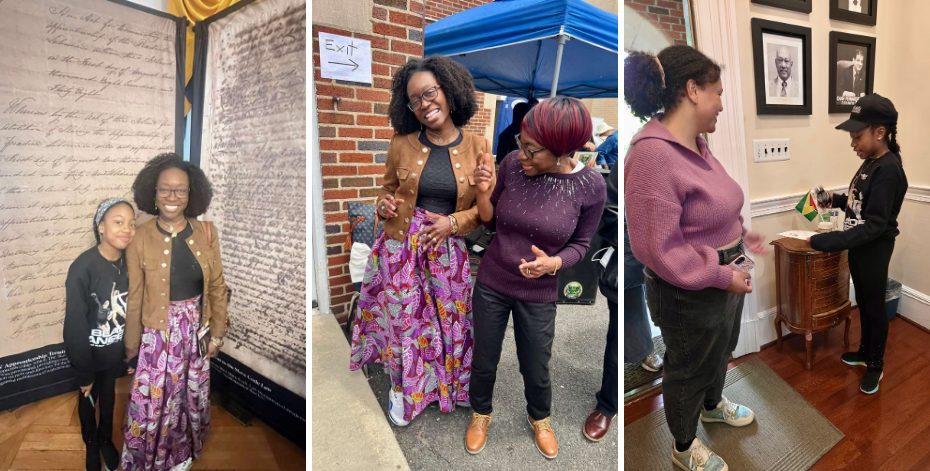
L to R: Ishara Lacsina and Executive Director Dr. Odessa Lacsina in the Embassy of Barbados; Dr. Lacsina shares a moment with her mother Celeste while celebrating at the Guyana embassy; Ishara volunteers at the Guyana embassy, greeting visitors.

Science Made Simple: Your Depression Might Have a Hidden Physical Cause You Can Actually Fix
EVIDENCE TO ACTION | Science Made Simple | The State of Women Institute
By Dr. Odessa Lacsina, Executive Director, The State of Women Institute
If you are struggling with depression, anxiety, or mood disorders and treatments are not working, there is something your doctor might be missing.
A study published in JAMA Network Open in December 2025 followed more than 30,000 people for nearly three years and found that people at high risk for sleep apnea had 40% higher odds of poor mental health — both at the time of the study and at the three-year follow-up.
The connection between sleep apnea and mental health is not new. What this study adds is scale, duration, and a finding that should change how we approach treatment-resistant depression and anxiety, particularly in women.
What Is Sleep Apnea?
Obstructive sleep apnea (OSA) causes repeated breathing interruptions during sleep. The airway narrows or collapses, cutting off oxygen — and a person may partially wake hundreds of times a night without knowing it.
The result is fragmented sleep, oxygen drops, stress responses, and chronic inflammation. And here is the part that surprises most people: up to 90% of people with sleep apnea don't know they have it. Nearly 936 million adults worldwide are affected, but most remain undiagnosed — often dismissed as simply snoring too much or feeling tired.
The Mental Health Connection
Lead researcher Dr. Tetyana Kendzerska and her team at Ottawa Hospital Research Institute found that sleep apnea significantly increases the risk of depression, mood disorders, anxiety disorders, and psychological distress — with depression showing the strongest link.¹
Among participants who began the study without any mental health conditions, those at high risk for sleep apnea had 20% higher odds of developing mental health problems by the three-year follow-up.
In other words, sleep apnea does not simply coexist with mental health issues. The evidence suggests it may actively cause or worsen them over time.
Why This Especially Matters for Women
Women are significantly underdiagnosed with sleep apnea because the condition presents differently across sexes.
Men typically experience: Loud snoring, gasping, obvious breathing pauses.
Women often experience: Insomnia, fatigue, morning headaches, depression, and anxiety — symptoms that are frequently dismissed as stress or hormonal fluctuation rather than investigated as signs of a sleep disorder.
If you are a woman being treated for depression or anxiety without improvement, it is worth asking your doctor specifically about sleep apnea screening.
The STOP Questionnaire: A Simple Self-Screen
The STOP questionnaire is a validated clinical screening tool. If you answer yes to two or more of the following four questions, you may be at high risk for sleep apnea and should speak with your doctor about a sleep study:
S — Snore: Do you snore loudly?
T — Tired: Do you often feel tired, fatigued, or sleepy during the day?
O — Observed: Has anyone observed you stop breathing during sleep?
P — Pressure: Do you have, or are you being treated for, high blood pressure?
Two or more yes answers is a reason to follow up. A sleep study can now be done at home in many cases — no overnight lab visit required.
Why the Connection Makes Sense
When sleep apnea goes untreated, the body undergoes a nightly cascade of stress. Intermittent oxygen drops deprive the brain of what it needs to function. Sleep fragmentation prevents the restorative deep sleep during which the brain processes emotions and consolidates memories. Chronic inflammation alters brain chemistry. Cortisol surges through the night, keeping the stress response in sustained overdrive. And the neurotransmitters that regulate mood — serotonin and dopamine — are disrupted.
This is not simply a matter of being tired. The brain is being stressed, repeatedly, night after night, with no recovery.
What You Can Do
Start with the STOP screening above. If you score two or more, talk to your doctor about a sleep study. Many studies can now be completed at home.
Treatment typically begins with CPAP therapy — a mask that keeps the airway open during sleep — though alternatives exist for mild to moderate cases, including oral appliances, positional therapy, and in some cases, surgical options. The first step is getting an accurate diagnosis.
If you are struggling with depression, anxiety, or mood symptoms — especially if current treatments have not been effective — sleep apnea is worth ruling out. It is a real, physical condition with real mental health consequences. And it is treatable.
Have you or someone you know been screened for sleep apnea?
Source
¹ Kendzerska, T., et al. "Obstructive Sleep Apnea Risk and Mental Health Conditions Among Older Canadian Adults." JAMA Network Open, December 26, 2025. Ottawa Hospital Research Institute. https://doi.org/10.1001/jamanetworkopen.2025.49137
Study population: 30,097 adults ages 45–85, followed for a median of 2.9 years.
Dr. Odessa Lacsina is the Executive Director of The State of Women Institute, a 501(c)(3) nonprofit working across three health equity pillars: Mental Health & Wellness, Maternal Health Equity, and Preventive Wellness.
To learn more or support women's health leadership, visit thestateofwomen.org or follow @thestateofwomen.

The Relationship Architect: Dr. Darlene Williams-Prades on Turning Personal Wounds into Generational Healing

Dr. Darlene Williams-Prades has a personal credo: born to serve, built to endure, called to inspire. Over thirty years of service — from the Air Force to federal leadership to the relationship strategy sessions where she has, more than once, used her own money to make sure a struggling client got a meal — she has lived every word of it.
6 UNIVERSITIES · 4,000+ LIVES TRANSFORMED · 30+ YEARS OF SERVICE · 8 BOOKS IN 2026
Born to serve. Built to endure. Called to inspire.
Dr. Darlene Williams-Prades has been living these words since long before she put them into language. They are her personal credo — forged across six decades of loss, service, resilience, and purpose — and they are the clearest map she has ever found to who she is and what she does.
From orphaned child to Bowie State University and Strayer University graduate, from Air Force veteran to federal leader, from entrepreneur to international coach, the arc of her life is remarkable in its consistency: every chapter has been, in some form, about showing up for people who needed her.
She serves as a concierge relationship strategist working with couples on the verge of separation or divorce, with corporations whose staff lacks effective communication, and with individuals navigating their own most difficult seasons. Her work bridges the distance between surviving life's challenges and thriving through them — helping build the kinds of relationships that can weather any storm.
She also serves on the FEMA Diversity and Inclusion Council, has authored multiple books including the forthcoming I Know Who God Made Me (May 2, 2026), and is building what she calls a generational legacy of service for her three children and four grandchildren.
Born to Serve
She was an orphaned child who had to learn, early and without the usual support, how to take care of herself. It would have been enough simply to survive that. Instead, it became the first chapter of a life defined by service to others facing exactly that kind of vulnerability.
Through her years in the Air Force defending her country, through her work in federal leadership, and into her current work transforming relationships and developing safety technology for underserved populations, Dr. Williams-Prades has never stopped moving toward the people who need her most. Every challenge she has faced, she says, deepened her understanding of what it actually means to serve.
Built to Endure
She lost both parents at sixteen. She has faced significant health challenges as an adult. In another life — or another temperament — any one of these experiences might have been the end of the story. For Dr. Williams-Prades, each one became preparation.
Her capacity to sit with people in their most difficult moments is not clinical distance. It is the recognition of someone who has been there. When she tells a client that the worst of what they are going through can become the foundation of something larger, she is speaking from a life that has proven it.
Called to Inspire
Eight books releasing in a single year. Speaking engagements. Safety technology in development for people who currently have no adequate protection. A relationship practice her clients describe as radical.
Dr. Williams-Prades' calling to inspire is not one thing. It shows up wherever there is a gap between what people are living and what they deserve. Her work across all of these dimensions carries the same conviction: that transformation is possible, and that the most credible guide through difficulty is someone who has already walked it.
Building a Legacy Through Service
Each company Dr. Williams-Prades has founded was built to close a gap — in how people relate to one another, and in how the most vulnerable among us are protected. Superior Love Forever, LLC addresses the first. Invisible Me, LLC addresses the second.
Superior Love Forever: Concierge Relationship Transformation
Dr. Williams-Prades works with couples on the verge of separation or divorce, with organizations whose staff lacks effective communication, and with individuals who need help understanding their own situations. What she offers is not traditional counseling — it is comprehensive transformation that holds the whole person, and the whole relationship system, in view at once.
She has used her own money to send struggling clients to spas. She has bought meals for people too overwhelmed to feed themselves. She calls it radical care. Her clients might call it the first time anyone told them, through action rather than words, that they were worth someone else's investment.
Invisible Me: Safety Innovation for the Underserved
Invisible Me, LLC began where so much of Dr. Williams-Prades' work begins: in personal experience of what it means to be unprotected. She is currently developing a safety device for underserved populations — particularly older adults and people with disabilities — because she knows from the inside what it costs a family to be without adequate protection.
The company is also, in her words, an act of love. Every innovation is designed with her grandchildren in mind, including one beloved grandchild on the autism spectrum, and every family that has ever known the particular fear of being without protection. The commitment behind it is straightforward: No family should have to live with the vulnerability and helplessness she has known.
She has known that fear. She intends to make sure others don't.
Recognition & Leadership
Awardee, Commander of the Most Noble Order of Global Peace Ambassadors (CGPA), appointed by WOLMI, a United Nations-accredited NGO with civil society programs in Geneva
Graduate, WOLMI Diplomatic Academy in Association with CICA International University and Seminary
FEMA Diversity & Inclusion Council Member
Air Force veteran
Author, I Know Who God Made Me (May 2, 2026) and 7 additional titles releasing in 2026
International Coach · Speaker · Entrepreneur
6 Universities served
30+ Years of Service
Where Her Work Meets Ours
The State of Women Institute works across three health equity pillars: Mental Health & Wellness, Maternal Health Equity, and Preventive Wellness. Dr. Williams-Prades' work touches every one of them, often simultaneously.
The faith-based relationship healing at the core of her practice addresses root traumas and builds the kind of emotional resilience that mental health systems alone rarely achieve. Her work with couples and families creates protective conditions for mothers navigating some of the most vulnerable periods of their lives, conditions that research consistently links to better maternal health outcomes. And her broader approach to resilience-building, which treats the whole person rather than the presenting crisis, does what the best preventive care does: it works upstream, before the emergency arrives.
None of it is labeled as health equity work. She is not running a clinical program. She is doing the quieter, more durable work of helping people stay intact in their relationships, in their families, and in themselves. That has always been health infrastructure. Dr. Williams-Prades has simply been building it for thirty years.
"When I first encountered Dr. Williams-Prades' work, I was struck by how she embodies the very principles she teaches about transformation. Here is a woman who turned losing both parents at sixteen into a calling to ensure no one else feels abandoned — who transformed personal health challenges into expertise that serves thousands. Dr. Williams-Prades offers something transformative: the lived experience of surviving abandonment and choosing connection, of facing vulnerability and building protection for others. Her work demonstrates that the most powerful health equity solutions come not from theory, but from the courage to transform our greatest challenges into our most meaningful service."
— Dr. Odessa Lacsina, Executive Director, The State of Women Institute
Learn more about Dr. Williams-Prades’ work at www.superiorloveforever.com
The State of Women Institute · thestateofwomen.org · @thestateofwomen
Science Made Simple: What Motherhood Does to the Brain (and Why It Matters)
EVIDENCE TO ACTION | Science Made Simple Mother's Day Edition | The State of Women Institute
By Dr. Odessa Lacsina, Executive Director, The State of Women Institute
This Mother's Day, we honor all the ways mothering shows up in our lives.
For those who've given birth. For those raising children not born to them. For those who've lost their mothers too soon. For those who've lost babies they'll never stop loving. For those waiting, hoping, and navigating the complicated terrain of becoming a parent.
And for those who mother in ways the world doesn't always count: aunts, teachers, mentors, chosen family.
Today's science recognizes what many have known all along: motherhood fundamentally changes you. And those changes last a lifetime.
The Research That Changed Everything
A groundbreaking study published in Scientific Reports analyzed brain scans from over 19,000 women aged 45 to 82. Lead researcher Valentina Rotondi and her team, working across multiple European institutions, wanted to answer a question that had never been asked at this scale:
Do the brain changes of motherhood endure for decades?
The answer was unequivocal: Yes.
Mothers showed widely distributed higher gray matter density compared to women who had never given birth, particularly concentrated in the frontal and occipital regions — areas involved in empathy, understanding others' emotions, and processing social information.
Here is what's remarkable: The brain scans were taken decades after these women had given birth. The youngest participant was 45. The oldest was 82. Yet the structural changes remained visible, measurable, and undeniable.
And fathers? No corresponding brain changes were observed. This transformation appears unique to those who carry, birth, and biologically mother children.
The study also found that both mothers and fathers reported a higher sense of life's meaning compared to those without children — but only mothers showed the corresponding structural changes in the brain.¹
What This Means
For years, mothers have described feeling fundamentally different after having children — not just behaviorally, not just emotionally, but in some deeper, harder-to-name way.
"I'm not the same person I was before."
Science now confirms it. The brain has been restructured. And those changes don't fade with time — they become part of who you are, woven into the architecture of your mind.
For Those Who Grieve
We want to acknowledge something important: this research studies those who gave birth and raised children. But mothering — and the love that drives it — exists in many forms.
If you've lost your mother, her impact on your brain is real. The neural pathways formed in childhood, shaped by her care, remain part of you.
If you've lost a child — whether through miscarriage, stillbirth, or after years together — you are a mother. Your body changed. Your brain changed. That transformation doesn't disappear with loss. The love remains, and so does the biological evidence of mothering.
If you're waiting to adopt, fostering, or raising children not born to you, you are mothering. While this particular study focused on biological birth, emerging research suggests that caregiving itself reshapes the brain — that the act of nurturing, of being attuned to a child's needs, creates its own neural adaptations.
The Complexity of Meaning
The researchers found that motherhood was associated with a higher sense of life's meaning. But this finding deserves care.
Meaning isn't a competition. Women without children — by choice or circumstance — live profoundly meaningful lives. The study shows an association, not a judgment.
For some mothers, that meaning comes mixed with struggle, exhaustion, grief, or regret. Motherhood is not universally joyful, and finding it difficult doesn't make you less of a mother or your brain changes less real.
The brain changes are a biological fact. The meaning is personal, complex, and yours to define.
Why This Research Matters
Understanding that the brain undergoes permanent restructuring during motherhood helps explain why postpartum mental health support is so critical. You are not "bouncing back." You are becoming someone new.
For aging and dementia research, these enduring brain changes may offer insights into protective benefits and long-term maternal mental health. For the women who have always said they were changed by motherhood — science now backs them up. This isn't weakness. It's transformation.
Motherhood, in its many forms, leaves an imprint — on the brain, on the body, on the heart, on who you become and who you'll be for the rest of your life.
This Mother's Day, we honor that transformation wherever it appears: in those who've given birth, in those who've adopted or fostered, in those who mother in ways uncounted, and in those who carry both the love and the loss.
The science shows us what mothers have always known: you never go back to who you were before. And maybe that's exactly how it should be.
To all the mothers, in all the ways that word can mean: We see you.
Source
¹ Rotondi, V., et al. "Enduring maternal brain changes and their role in mediating motherhood's impact on well-being." Scientific Reports, Vol. 14, July 18, 2024. https://doi.org/10.1038/s41598-024-67316-y
Study population: 19,043 women and 17,612 men aged 45–82, drawn from the UK Biobank.
Dr. Odessa Lacsina is the Executive Director of The State of Women Institute, a 501(c)(3) nonprofit working across three health equity pillars: Mental Health & Wellness, Maternal Health Equity, and Preventive Wellness.
To learn more or support women's health leadership, visit thestateofwomen.org or follow @thestateofwomen.

The Breathwork Healer: Melissa Losito Braithwaite on Sisterhood, Trauma, and Learning to Breathe Again

For most of her life, Melissa Losito Braithwaite was afraid to breathe. Now she has built a practice — and a community — around helping other women do exactly that.
40 YEARS FROM TRAUMA TO PURPOSE · 4 SESSIONS TO END FLASHBACKS · 1 SESSION TO UNBLOCK YEARS OF TRAUMA · 11: AGE WHEN SHE RECEIVED HER SACRED ASSIGNMENT
A Life Shaped by Breath
There was a moment that shaped everything. At age four, Melissa Losito Braithwaite was found blue at the bottom of a pool, requiring CPR from her father to bring her back to life. That near-drowning left her with a profound awareness that death could happen at any moment — and a family too traumatized to help her process what had happened.
"From that day forward, I was always afraid to breathe incorrectly," she recalls. "Any kind of exercise or activity that changed my breathing from normal scared me very much." That fear would manifest as debilitating panic attacks that began during her college years at Immaculata University and continued throughout her career as a beloved third-grade teacher.
But trauma wasn't the end of Braithwaite's story — it was the beginning of her calling. Seven years after the near-drowning, at age eleven, something would set her on a path that would take 40 years to fully understand.
A Sacred Assignment
During a family bingo night at her Catholic school, something drew eleven-year-old Braithwaite to the empty church next door. Kneeling in the front pew, she experienced what she describes as "the most encompassing, loving feeling I ever felt in my life." In that moment of stillness, she heard words that would stay with her for decades:
“Melissa, you have something important to do in this lifetime with me.”
— The message Melissa Losito Braithwaite heard at age eleven
That sense of a divine mission followed Braithwaite through everything: her degree in elementary education from Immaculata University in 1992, her years as a teacher, her marriage in August 1997, and her journey into motherhood with daughter Grace — born in 2002 after six years of trying — and her son, born in 2007. Through postpartum depression, through persistent panic attacks that no medication could touch, through years of searching for her true purpose, that sense of calling remained constant.
The Long Journey Home
Braithwaite’s spiritual seeking led her on an extraordinary journey of discovery — solo retreats to Tahiti and Costa Rica, certifications in Reiki healing and crystal therapy, Kundalini yoga teacher training in Norway. Each experience expanded her understanding of healing, but none quite fulfilled the calling she had felt since childhood.
Conventional medical approaches had, by her account, largely failed her. Psychiatrists prescribed medications that didn't work. Specialists at Jefferson Headache Center couldn't resolve her migraines. Therapists offered little in the way of lasting relief. "There was a therapist who said, 'Oh, there's a book you should read. It's called the Panic Attack Disorder book,' and that was the end of that," she remembers.
In 2021, after a stage 0 breast cancer diagnosis and lumpectomy, Braithwaite's search intensified. She had already begun volunteering with Pennies in Action, a 501(c)(3) nonprofit supporting the DC1 immunotherapy breast cancer research of Dr. Brian Czerniecki, but something was still missing. At a retreat in Costa Rica, she experienced her first breathwork session — and despite her long-held terror of altered breathing, felt something shift.
Learning to Breathe Again
Months after that first session, and despite her fear, Braithwaite reached out to breathwork teacher and trainer David Elliott. At his 2022 training at the Omega Institute in New York, she was so frightened she couldn't lie down. With tears streaming down her face, she told him she didn't think she could do it.
Elliott, a farmer from Kentucky, was matter-of-fact: "Oh, you'll be fine. Just lay down and start the breathwork." That calm reassurance changed the direction of what followed. By the fourth day of training, Braithwaite says, something shifted in how she understood the drowning incident. After that session, she reports, she never had another flashback.
“I realized: I need to do this. This is what people need to learn about. This is what I need to share with other people.”
— Melissa Losito Braithwaite
Healing Through Sisterhood
Today, Braithwaite facilitates breathwork sessions that combine personal healing with community — what she calls gathering women together in sisterhood. In her practice, breathwork works with what she describes as stored emotional tension in the body, but she is equally focused on what happens in the room after the breathing ends: the conversations, the recognition, the sense of not being alone.
"We don't have that anymore, and it is so needed," she says. "A lot of the healing happens when we release through breath, but healing also happens when you connect with other women."
The responses she witnesses in her sessions are varied. A poet laureate who hadn't written in years created a poem after a single session. Participants describe releasing emotions they had carried for decades. Women reconnect with creativity and a sense of self they thought they had lost.
"Our job in life is to be authentic and express ourselves authentically, to be creative and be in flow," Braithwaite says. "When we can do that, we're living joyfully. Breathwork helps us connect back to our true self, our essence, our spirit. It's a shortcut to healing, a shortcut to your inner child."
Training & Certifications
Immaculata University, Elementary Education (1992)
Certified Breathwork Healer, David Elliott Training
Reiki Healing Certification
Crystal Healing Certification
Kundalini Yoga Teacher Training (Norway)
ICE Works Homeschool Education (1998–2001)
Pennies in Action Volunteer (Supporting DC1 Immunotherapy Research)
Third Grade Teacher (1992–1997)
Where Her Work Meets Ours: Breath as Health Infrastructure
The State of Women Institute works across three health equity pillars: Mental Health & Wellness, Maternal Health Equity, and Preventive Wellness. What draws us to Braithwaite's work is its focus on the whole person — not as a substitute for clinical care, but as a complement to it, and as an approach to the emotional and communal dimensions of wellness that conventional systems often leave unaddressed.
Her breathwork practice works with trauma, anxiety, and panic — the very conditions she navigated for decades herself — and her approach is grounded in the understanding that healing is rarely a solitary process. Having lived through postpartum depression, Braithwaite brings firsthand knowledge to the isolation many new mothers face, and her sisterhood model offers something that clinical settings rarely can: sustained community.
Her advocacy and volunteerism with cancer research organizations reflects the same conviction that whole-person wellness and evidence-based medicine are not in opposition. For Melissa, they are part of the same continuum.
Pillars: Mental Health & Wellness · Maternal Health Support · Preventive Wellness · Trauma Healing
Building the Future of Healing
Melissa's vision extends beyond individual sessions. She is working toward regular gatherings where women can come together to breathe, release, and reconnect — and her partnership with The State of Women Institute's upcoming wellness network is aimed at making these experiences accessible to women across a broader range of communities.
"Whatever stage of life in which women find themselves, we are all holding onto energy and emotions that no longer serve us," she says. "This takes up space in our bodies that we don't need to hold on to anymore. When we release it, we make space for our innate creative spark. When women gather and experience this together, something magical happens. Women become sisters almost immediately, as we are able to see ourselves and each other as we truly are."
From the four-year-old who nearly drowned to the healer now teaching women to breathe freely again — Melissa's path has been shaped at every turn by the very experiences she once feared most. What she found on the other side of that fear became her life's work.
“Melissa’s work demonstrates that true preventive wellness isn’t just about avoiding illness, it's about helping women reconnect with their essential selves, their breath, and each other. In a world where women often hold their trauma in silence, Melissa creates a sacred space where healing happens through both breath and sisterhood.”
— Dr. Odessa Lacsina, Executive Director, The State of Women Institute
Connect with Melissa Learn more about Melissa's breathwork practice and upcoming gatherings.
www.melissalosito.com · @melissaslosito
The State of Women Institute · thestateofwomen.org · @thestateofwomen
Counting What Matters: Women Leading Health Equity in Guyana

The work of health equity is often described in terms of systems, policies, and outcomes. But in Guyana, I was reminded that it is first and foremost about people – and women, in particular – who carry the weight of those systems while quietly reshaping them.
By Dr. Odessa Lacsina, Executive Director, The State of Women Institute
I arrived in Guyana's capital of Georgetown just as International Women's Day was being celebrated around the world. The timing felt symbolic, but what unfolded over the following days offered an instructive view of how women lead — not in ideal conditions, but within the real constraints of geography, resources, and history. I traveled as a health equity advocate, hoping to better understand how women navigate these constraints. What I found, consistently, were resilient women leaders taking action to build systems of care where gaps still exist, and doing so with clear focus on what their communities need most.
Leadership at Every Level
My meeting with Guyana's First Lady, Arya Ali, took place on a Friday evening during a Ramadan festival near Georgetown's historic sea walls. I brought my daughter with me, wanting her to witness the importance of cultural respect and global connection. As the First Lady and I spoke about women's health, policy, and prevention, one idea she shared stood out:
“Health doesn’t wait for perfect systems. Our women can’t wait for perfect systems either — they are creating solutions now.”

L to R: Dr. Odessa Lacina at the First Lady of Guyana (Her Excellency Arya Ali ) International Women’s Day March: Empowering and celebrating women everywhere. / Hon. Minister Vindhya Persaud with Ishara Lacsina at WeLife6 Expo, an entrepreneurship conference for women and girls. Minister Persaud is responsible for policy health equity government infrastructure and economic empowerment for women. / Ishara and Dr. Odessa Lacsina with Hon. Kwame W.E. McCoy, the Minister within the Office of the Prime Minister in Guyana.
That theme surfaced again and again throughout the trip. It was present in conversations with Ministry of Health officials designing preventive care strategies, and in discussions with women leading community-based initiatives. Across these settings, there was a consistent understanding: progress depends not only on formal systems, but on the women who navigate and strengthen them every day.
Where Policy Meets Practice
In meetings with the Ministry of Health, I saw what effective policy looks like when it is informed by lived experience and led by women focused on designing health interventions that account for the realities of distance, access, culture, and daily life. This kind of leadership is often overlooked because it does not always fit neatly into traditional measures of impact. Yet it is precisely this integration of clinical knowledge with community understanding that makes health systems more responsive and durable.
These partnerships also reflect the approach that guides our work at The State of Women Institute. Health challenges do not exist in isolation, and solutions cannot either. They must reflect the full context of women's lives.
The Wisdom of Communities
The clearest lessons came during my visits to community health sites. In one community, I met a woman who had lost her sister to preventable complications during childbirth. She now leads maternal health education efforts in her region, ensuring that other families have access to information and care that her own family did not. In another, a grandmother described how she teaches traditional healing practices while encouraging younger women to seek preventive health services. Her approach was not about choosing between health systems, but about bridging them.
These are not isolated stories. They reflect a broader pattern: women translating personal experience into collective action. Their leadership operates across multiple levels — within families, across communities, and alongside formal health institutions. This is how health systems evolve in practice — beyond policy directives and through the daily work of people who understand both the gaps and the possibilities.

Left: L-R: Martina McDonald-Johnson, Managing Director, Integrated Marketing Communications; Isahra Lacsina; Dr. Alista Bishop, finance executive and author of the recently published “The Journey of Alista Bishop,” McDonald-Johnson’s daughter. Middle: Dr. Odessa Lacsina with Hon. Oneidge Walrond, Minister of Home Affairs. Right: Dr. Odessa and Ishara Lacsina as guests at the 6th Annual Guyana Women & Girls Summit.
Shared Health Challenges: Local and Global
Traveling during International Women's Day underscored something that extends beyond any one country. The barriers women face in accessing care — whether shaped by distance, cost, or system navigation — are not unique. The conversations I had in Guyana about cervical cancer prevention, maternal health, and access to health screening echoed concerns I have heard in cities across the United States. The contexts differ, but the underlying challenge is the same: how to ensure that prevention, early detection, and care are truly accessible.
It is the specificity of local solutions that allows us to see connections between different health settings and to build strategies that are both locally grounded and globally informed. Meaningful progress depends on true partnership. The leaders I met in Guyana are not waiting for external solutions — they are already advancing them. What they seek are partners who will listen, support, and help extend the reach of what is already working. Their leadership makes clear what is required next: investment, infrastructure, and sustained partnership.
This is the role The State of Women Institute is committed to playing.

Participants join First Lady Arya Ali, Minister of Human Services and Social Security Dr. Vindhya Persaud, and other Cabinet members for a vibrant walk through Georgetown in celebration of International Women’s Day. The event, which began at the Bank of Guyana and concluded at the Kingston Seawall Esplanade, symbolized unity, empowerment, and collective commitment to advancing the rights and wellbeing of women across Guyana.
Photo courtesy of the Ministry of Human Services and Social Security.
Our partnership with Guyanese health leaders will focus on amplifying existing efforts while contributing resources, platforms, and connections. The Healing Roots initiative will incorporate insights from culturally responsive prevention strategies. Our podcast network will create space for Guyanese leaders in women's health to share their work with global audiences. Our research translation efforts will highlight community-based models that can inform broader approaches to care in similar settings. The State of Women Institute's goal is to shine a spotlight where health innovation already exists — and to ensure it is supported and sustained.
Moving Health Equity Forward
As I departed Guyana, I reflected on the determined, transformative work I had witnessed. There was no sense of pause. The same women I had met would return the next day to their responsibilities — coordinating care, educating families, shaping programs, and advocating for improvements. Their efforts are already transforming health outcomes in ways that may not always be visible at scale, but are deeply felt within their communities.
The lesson from Guyana for International Women's Day is straightforward: when women lead, health systems become more responsive. When their leadership is supported, those systems become stronger. And when their insights are shared across contexts, the impact extends far beyond any single setting.
This is the kind of progress The State of Women Institute champions — not only on International Women's Day and during Women’s History Month, but on every day that follows.
Dr. Odessa Lacsina is the Executive Director of The State of Women Institute, a 501(c)(3) nonprofit working across three health equity pillars: Mental Health & Wellness, Maternal Health Equity, and Preventive Wellness. The State of Women Institute's work spans from Baltimore to international partnerships, always centered on amplifying women's voices and building the infrastructure to support community-led health solutions.
To learn more or support women's health leadership globally, visit thestateofwomen.org or follow @thestateofwomen.

Unequal Pay, Unequal Health: The Hidden Health Costs of the Pay Gap
Equal Pay Day was yesterday. The date is a calculation, but the consequences are daily: smaller paychecks shape choices that affect women’s mental health and family life. This piece explains how the numbers translate into stress, what the evidence shows about income and mental health, and which policy changes have the clearest support.
When Equal Pay Day arrives, the story is often a single statistic and a single headline. The calculation is simple: how far into the new year women must work to earn what men earned the year before. The date landed yesterday. The underlying figures did not change overnight. According to the U.S. Census Bureau, the female‑to‑male earnings ratio for full‑time, year‑round workers was 80.9 percent in 2024. The Bureau of Labor Statistics reports median weekly earnings in the fourth quarter of 2024 were $1,083 for women and $1,302 for men. Analysts at the Institute for Women’s Policy Research and the Economic Policy Institute show the gap is larger for Black and Latina women and that controlled measures widened again in 2025.
Those numbers matter in small, practical ways. A few hundred dollars a month can determine whether a family keeps a childcare slot, fills a prescription, or pays for a therapy visit. The American Psychological Association’s Stress in America surveys place money and the economy among the top stressors for adults, and women report higher levels of money‑related strain. Over time, the choices people make to stretch a paycheck accumulate into chronic stress that affects sleep, concentration, and mood.
When extra income changes health
Researchers have asked whether income itself moves mental‑health outcomes. A 2023 systematic review in PLOS One examined randomized and quasi‑experimental cash‑transfer programs and found modest but consistent reductions in depression and anxiety, with larger effects for unconditional payments. Those studies suggest that when money reaches households in need, mental‑health symptoms can fall while the support continues.
Evidence from high‑income settings is more mixed, and that matters for policy design. A 2024 study in JAMA Network Open that analyzed state minimum‑wage changes and children’s mental health found no clear, consistent improvements across a broad set of outcomes. The JAMA analysis shows that the size, duration, and targeting of income changes determine whether health outcomes shift. Small or temporary increases rarely produce the same effects as sustained, well‑targeted supports.
From these findings two practical points follow. Income can be a lever for mental‑health improvement when it reaches the households that need it. Policy must be designed to reach those households consistently and at sufficient scale.
The unpaid work that deepens the squeeze
Earnings are only half the picture. Time‑use data from the Bureau of Labor Statistics and reporting from the Pew Research Center show women still shoulder more childcare, eldercare, and household tasks. The National Partnership for Women & Families estimates unpaid care in the United States is worth more than $1 trillion annually, and women perform roughly two‑thirds of that labor.
That unpaid work pushes many women into part‑time or lower‑benefit jobs. Those positions often lack employer mental‑health coverage and paid leave. Recent analyses from 2023 to 2025 document higher rates of burnout among working mothers and a greater likelihood of leaving paid work because of caregiving demands. Over a career, interrupted earnings and missed promotions compound into large lifetime losses. The National Women’s Law Center reports that the median annual earnings gap in 2024 translated to roughly $13,570 less per year for a woman working full time compared with a man, and lifetime losses can exceed half a million dollars over a 40‑year career, with larger shortfalls for women of color.
A small sensory detail can make the arithmetic feel immediate: in a clinic waiting room, the faint smell of coffee and the rustle of a folded prescription receipt in a trash can can stand for the choice between medicine and groceries. That scrap is a quiet record of tradeoffs that accumulate into chronic stress.
How families feel the impact
Lower earnings change household choices in concrete ways. Analyses from the National Women’s Law Center and other groups show that wage gaps reduce spending on essentials such as healthcare, childcare, and nutritious food. The Kaiser Family Foundation’s surveys on women’s health document gaps in affordability and access for mental‑health services. When families delay preventive care or skip therapy because of cost, conditions that could have been managed early become harder to treat.
Public‑health literature links parental financial strain to children’s emotional and behavioral outcomes. Children raised in households with chronic economic stress show higher rates of anxiety and behavioral challenges, and those effects can persist into adolescence and adulthood. The cumulative pattern is both economic and psychological: decades of smaller paychecks, interrupted careers, and deferred care shape how households plan, how parents divide labor, and how children experience stability.
What fair pay would change, practically
If pay were fairer tomorrow, the effects would be practical and measurable.
More reliable access to care. Evidence from cash‑transfer studies shows reductions in depression and anxiety when households receive sustained income boosts. Even modest, reliable increases in income can make therapy, medications, and preventive visits affordable rather than optional.
Fewer tradeoffs between work and care. Fairer wages reduce the pressure to choose between childcare and a paycheck or between groceries and a prescription. That reduces decision fatigue and the chronic stress that contributes to burnout.
Caregiving becomes more manageable. With higher earnings, families can afford childcare, eldercare, or a few hours of paid help. That breathing room changes the rhythm of daily life and reduces emotional exhaustion.
Children grow up in calmer homes. Reduced parental stress improves children’s emotional stability, school attendance, and long‑term outcomes.
Communities gain. Higher earnings for women strengthen local economies, stabilize housing, and increase demand for services that support family health.
These outcomes depend on policy design. The JAMA Network Open study on minimum wages shows that raising wages alone does not guarantee mental‑health improvements for children. Policies that combine pay equity with caregiving supports—paid family leave, affordable childcare, pay transparency, and targeted income supports—are more likely to reach the households that need them.
Policy levers with evidence
Several policy tools have empirical support and practical logic.
Pay transparency and audits. Requiring employers to disclose pay ranges and conduct equity audits helps workers identify and correct unexplained wage differences.
Paid family leave and childcare subsidies. These reduce career interruptions that drive lifetime earnings losses and give families predictable options for care.
Targeted income supports. Refundable tax credits and child allowances lift household incomes directly and have shown mental‑health benefits in multiple studies.
Stronger enforcement of equal‑pay laws. Better enforcement can correct systemic disparities that accumulate over careers.
Equity must be central. The Institute for Women’s Policy Research and the Economic Policy Institute show the wage gap is largest for Black and Latina women. Policies that ignore race and caregiving status will leave the most affected groups behind.
How to keep the conversation going
Publishing the day after Equal Pay Day gives this piece a different shape. The date is a prompt. The work that follows is sustained. Yesterday’s headlines remind readers that the calculation exists. Today’s reporting should push beyond the ritual and into the evidence: how pay affects mental health, which policies have shown results, and which communities face the deepest losses.
Track a few indicators. Watch median earnings by gender and race. Watch mental‑health surveys that break out results by caregiving status and income. Watch evaluations of policy pilots—paid leave programs, childcare subsidies, and targeted cash supports—that measure mental‑health outcomes. Those indicators will show whether the conversation moves from a single day to lasting change.
Journalists and advocates can help by telling the stories behind the numbers. Profiles of families who face the tradeoffs between care and work make the stakes tangible. Reporting that connects wage policy to mental‑health outcomes will broaden the conversation beyond paychecks and into the daily lives of women and children.

The Media Visionary: Dr. Vonnya Pettigrew on Building an Empire — and a Community — from the Ground Up

There is a building on the waterfront of Baltimore's Canton Harbor that tells a story most people never expected to be told. At 2220 Boston Street, on a 14,400-square-foot block of prime Maryland waterfront real estate, a Black woman from Baltimore built an empire — not with investors, not with grants, not with programs. She built it with vision, discipline, and an unshakeable belief that the communities she served deserved to see themselves reflected not just in stories, but in the very infrastructure that tells those stories.
27+ YEARS IN MEDIA · 7 BUSINESS VENTURES · 14,400 SQ FT WATERFRONT · K–12 YOUTH VIA FILM ACADEMY
The Foundation
That woman is Dr. Vonnya Pettigrew, HonD — CEO and founder of Root Branch Media Group, Honorary Doctorate recipient in Business Philosophy, former White House intern, award-winning filmmaker, and one of the most quietly powerful forces at the intersection of media, community development, and health equity in the mid-Atlantic region.
The State of Women Institute started Architects of Wellness to document something specific: what it actually looks like when women build health equity infrastructure rather than just describe it. In Baltimore, Dr. Pettigrew has been doing exactly that since 2006.
From White House to Waterfront
Dr. Pettigrew was an intern in the White House Speech Writing Department under President Bill Clinton in 1999 when she got her first real lesson in how power communicates. She got a front-row seat to the most powerful communications operation in the world. She watched how language shapes policy, how narrative moves people, and how the stories told in the halls of power determine whose lives are centered — and whose are left at the margins.
She returned to Baltimore with something most interns don't leave Washington with: a mission. Not just to tell stories, but to build the infrastructure that allows marginalized communities to tell their own.
In 2006, Dr. Pettigrew founded Root Branch Media Group. What started as a media production firm quickly evolved into something far more expansive — an ecosystem of interconnected businesses and nonprofits designed to address the full landscape of what communities need to thrive: media, economic opportunity, youth development, workforce training, and underlying all of it, the health and wellbeing of the people she serves.
“My vision is to educate, equip, and empower others to control their narratives in a world where their stories are often told for them or shaped by stereotypes or societal norms.”
— Dr. Vonnya Pettigrew, HonD
The Root Branch Multiverse
To understand Dr. Pettigrew's impact on community wellness, it helps to understand the breadth of what she has built. Root Branch Media Group is not a single company — it is an ecosystem. Each branch addresses a different dimension of community need, and together they form something most communities in America desperately lack: locally owned, community-serving infrastructure.
Root Branch Media Group Award-winning production firm delivering video, film, branded content, animation, and photography — with credits including Discovery Channel, TV One, MPT, and Charm TV.
Root Branch Film Academy Film and digital media arts education for youth K–12, giving young people creative tools, career pathways, and a reason to believe their stories are worth telling.
Root Branch Marketplace A home-shopping style television series spotlighting local Maryland small businesses from all across the state, training entrepreneurs in digital media, marketing, and the tools to scale in the digital economy.
Root Branch G.R.O.W. Professional training and workforce development for adults 18+ — building economic opportunity for those who need it most in the mid-Atlantic region.
Root Branch Arts & Outreach Institute A 501(c)(3) nonprofit ensuring arts education and community programming reach those who might otherwise be left out of cultural and creative life.
Root Branch Press Coffee & Co. A forthcoming community gathering space — because wellness requires places where people can come together, connect, and build belonging.
Each of these ventures does something no single awareness campaign could: It creates a permanent structure that continues to serve the community long after any given initiative ends.
Why Media Is a Health Issue
When most people think about health equity, they think about access to doctors, insurance, and hospitals. Dr. Pettigrew thinks bigger. She understands something that research increasingly confirms: Whoever controls the narrative controls the conditions that determine health outcomes long before anyone walks into a clinic.
When Black communities don't see themselves in media — as entrepreneurs, innovators, healers, and leaders — it affects self-perception, aspiration, and the sense of possibility that shapes mental wellness at every stage of life. When young people have no creative outlets, no pathways to purpose, no structures that say their story matters, the mental health consequences are profound and lasting.
The Root Branch Film Academy doesn't just teach kids to make films. It tells them — with every lesson, every camera placed in their hands, every story they are asked to tell — that they are worth seeing. That their experiences are worth documenting. That they have something to say that the world needs to hear.Reframed in public health terms, this is preventive wellness: community mental health infrastructure built one student at a time through the daily work of telling young people that their stories matter.
“When women like Dr. Pettigrew build economic power, create platforms for storytelling, and invest in youth development, they are building health equity — whether they call it that or not.”
— Dr. Odessa Lacsina, Executive Director, The State of Women Institute
From the Statehouse to the Screen
Dr. Pettigrew's commitment to community wellness extends far beyond her businesses. As an active member of the National Coalition of 100 Black Women Baltimore Metropolitan Chapter, she has stood on the floor of the Maryland State Capitol to advocate for the health and rights of Black women and families. She has developed culturally responsive "Know Your Rights" campaigns for National Guard, law enforcement, and immigrant communities — understanding that health equity requires not just access to care, but access to the knowledge that protects lives.
This willingness to move between roles — filmmaker, entrepreneur, advocate, educator, policy voice — is what makes Dr. Pettigrew extraordinary. She refuses to be boxed in. She understands that the fight for Black women's health and wellbeing requires presence in every room where decisions are made.
Recognition & Leadership
25 Women to Watch 2025, The Baltimore Sun
Top 100 Women in Maryland, The Daily Record (2023)
Women of Vision Award, Women in Film & Video DC (2023)
Goldman Sachs 10,000 Small Businesses Program Alumni
Baltimore Leadership Class 2023 Alumni
Distinguished Toastmaster
Member: National Coalition of 100 Black Women · Black Leadership Circle · NABJ · BABJ · NAACP Baltimore
Baltimore City Chamber of Commerce · NAWBO DC · The CEO Club
The Women of Vision Award places Dr. Pettigrew in the company of legends: Cicely Tyson, Ruby Dee, Gwen Ifill, Penny Marshall, Tipper Gore — women who used their platforms to tell truth, challenge power, and open doors. Dr. Pettigrew belongs in that lineage, and she is just getting started.
Where Her Work Meets Ours
The State of Women Institute works across three health equity pillars: Mental Health & Wellness, Maternal Health Equity, and Preventive Wellness. What is most striking about Dr. Pettigrew's work is that it touches all three — not through programs explicitly labeled as "health," but through the deeper infrastructure that health equity requires.
Economic stability is a primary driver of mental wellness. Her Root Branch Marketplace and G.R.O.W. program build the economic foundation that reduces the chronic stress, anxiety, and financial trauma driving so many mental health disparities in Black communities. Youth with creative outlets, mentors, and structured pathways to purpose are profoundly less likely to experience the mental health crises that devastate young communities — making the Film Academy preventive mental health care at scale. And her advocacy at the Maryland State Capitol for Black maternal health is a reminder that the fight for health equity happens in every arena: not just in clinics, but in legislative chambers, community centers, and yes, on Baltimore's waterfront.
Pillars: Mental Health & Wellness · Economic Empowerment · Maternal Health Advocacy · Youth Development
What She’s Building Next
Dr. Pettigrew’s vision extends far beyond Baltimore. She has her eyes on building media arts hubs in urban communities across the country — spaces where young people of color can learn the craft of storytelling and the business of media, where entrepreneurs can build and grow, and where communities can gather and connect.
She is currently partnering with The State of Women Institute to bring health equity programming into the Root Branch ecosystem, from podcast production support to mentorship for the next generation of women health communicators — a collaboration rooted in a shared conviction that media infrastructure and health equity infrastructure are not separate conversations. They are the same conversation.
“These aren't just professional interests for either of us — they’re deeply personal missions rooted in the women we've loved and lost, and the generations we're determined to protect.”
— Dr. Odessa Lacsina, on the partnership between The State of Women Institute and Root Branch Media Group
Because when a Black woman owns the waterfront — when she controls the building, the platform, the camera, the story — she changes what is possible not just for herself, but for every woman and child who walks through her doors. That is health equity. That is systems change. That is what an Architect of Wellness looks like.
Connect with Dr. Pettigrew Follow Root Branch Media Group and support the work of women building health equity infrastructure in Baltimore and beyond.
Root Branch Media Group · rootbranchmediagroup.com · @rootbranchmg · @vonnyarooted
The State of Women Institute · thestateofwomen.org · @thestateofwomen
The Policy Architect: Alexis Solis on Building Health Equity from the Inside Out

For more than 15 years, Alexis Solis has been doing the unglamorous, essential work of equity — navigating bureaucracies, rewriting rules, and refusing to accept that the systems meant to serve marginalized communities must stay broken. Now she is bringing that same tenacity to the halls of Congress.
15+ YEARS OF ADVOCACY · $12B FEDERAL PORTFOLIO · MD-5 CONGRESSIONAL DISTRICT · 3 THE STATE OF WOMEN PILLARS ADVANCED
The Bridge Builder
Alexis Solis does not fit neatly into any one category — and she has learned to lean into that.
The daughter of a Nicaraguan and white father and a Black mother, she grew up navigating multiple worlds, learning early that identity is not a limitation but a lens. Today, as a book author, youth volleyball coach, Vice President of Government Relations at Tryfacta, CEO of Empress Consulting International, and congressional candidate for Maryland's 5th District, she brings that same multidimensional perspective to everything she touches: from healthcare policy to mental health advocacy to the youth volleyball court.
"I've always believed that leadership isn't about fitting into one lane — it's about building bridges across many," she says. "Whether it's healthcare policy, mental health advocacy, or mentoring young athletes, showing up fully and doing the work for my community — that's the job."
That perspective has shaped a career spanning three decades of advocacy — more than 15 of them focused on consulting, policy, and community leadership in Prince George's County, one of Maryland's most politically complex and historically underserved counties. Long before health equity became a national conversation, Solis was in the rooms where it was being neglected — making sure someone in those rooms was paying attention.
"Policy is health. If we want stronger communities, we have to write laws that treat health as a priority, not a privilege." — Alexis Solis
From Federal Corridors to Community Roots
Before joining Tryfacta, Solis founded Empress Consulting International (ECI), a firm dedicated to supporting small businesses from formation and certification through scaling, contracting, and long-term sustainability — both domestically and internationally. Prior to launching ECI, she managed a federal, state, and local portfolio exceeding $12 billion at 22nd Century Technologies, where she gained an intimate understanding of how federal resources flow, where they stall, and who bears the cost when they fail to reach the communities they were designed to serve.
She witnessed firsthand how federal health and social programs could be transformative in theory yet inequitable in practice, when implementation overlooked the realities on the ground.
That experience became the foundation of Empress Consulting International, where she works with small businesses, government agencies, nonprofits, and health systems to bridge the gap between federal intent and community reality. In addition to advisory and strategic consulting services, ECI also provides staffing support, connecting organizations with qualified professionals to ensure operational continuity and mission success.
Today, as vice president of government relations at Tryfacta — a California-based technology and staffing partner with 185 government contracts across the country — her work is focused on driving strategic growth, strengthening public-sector partnerships, and expanding national impact, while ensuring that policy, procurement, and community outcomes remain aligned.
When Health Policy Is Personal
For Solis, health equity has never been abstract. After losing her mother to mental health challenges, she joined the board of the National Alliance on Mental Illness (NAMI), turning grief into sustained advocacy. She has since championed efforts to expand access to care, reduce stigma, and confront the systemic barriers that disproportionately affect communities of color.
As federal budget debates place mental health funding at risk, she does not hedge: "We cannot strengthen communities while cutting the services that keep families stable. If funding is threatened, I will fight in Washington to protect it — because mental health care is essential."
Her work on the Special Education Advisory Committee reflects the same conviction: that education and health are not separate issues but deeply interconnected ones. And when she steps away from the policy table, she is on the volleyball court, mentoring young girls and helping them build the resilience, confidence, and sense of community that formal systems too often fail to provide.
Now, as a congressional candidate for Maryland's 5th District, Solis is carrying that same record into the political arena. Her platform centers on health equity, economic stability, educational equity, and inclusive representation for the diverse communities of Prince George's County and Southern Maryland.
Why Alexis Solis Opens Architects of Wellness
Every Monday, we introduce you to a woman who is building something — in policy, in medicine, in research, in community. We're calling the series Architects of Wellness, because the women we're highlighting aren't just advocates. They're constructing the infrastructure that health equity actually requires.
We're starting with Alexis Solis because her work makes something visible that often stays invisible: the direct line between policy decisions and the health outcomes of real people. The laws passed, the budgets allocated, the programs funded or defunded — these are not abstractions. They determine who survives and who thrives. Solis has spent decades inside those systems, and she understands that changing them requires exactly the kind of sustained, unglamorous, inside-out work that rarely makes headlines.
Health equity needs more than clinicians and researchers. It needs people who understand how power moves — and who are willing to go where it lives.
Where Her Work Meets Ours:
Pillar 1 — Mental Health & Wellness Advocating for mental health funding, parity legislation, and youth mental health in sports and schools.
Pillar 2 — Maternal Health Equity Championing maternal health policy reforms that address racial disparities, centering Black and Latina women.
Pillar 3 — Preventive Wellness Former board member of the BREM Foundation, advancing early detection, equitable screening, and cancer research funding.
Building What Must Exist
What distinguishes Solis is a relentless practicality. She is not interested in visibility for its own sake, in performative politics, or in advocacy that stops at awareness. She wants structures changed. Budgets rewritten. Programs redesigned. And she is deeply familiar with how tedious, unglamorous, and necessary that work is.
For the communities of Maryland's 5th District — and for every woman who has been failed by a health system that was never built with her in mind — Alexis Solis is building something different. Not just a platform. Infrastructure.
That is, after all, what architects do.
"Alexis understands something The State of Women holds at its core: the gap between health equity as a concept and health equity as a reality is a policy gap. We need architects in Congress — people who know how to read the blueprints and aren't afraid to rebuild what isn't working." — Dr. Odessa Lacsina, Executive Director, The State of Women Institute
Leadership & Service
Vice President of Government Relations, Tryfacta
CEO, Empress Consulting International
Congressional Candidate, Maryland's 5th District
Board Member, BREM Foundation to Defeat Breast Cancer
Special Education Advisory Committee Member
15+ Years of Prince George's County Advocacy
Youth Volleyball Coach
Member, Alpha Kappa Alpha Sorority, Inc. — Psi Phi Omega Chapter
Former Board Member, American Red Cross, Southern Maryland Chapter
Author, She Rose: A Story of Strength, Vision and Voice — https://a.co/d/0bY0WIE8
Connect with Alexis Solis Website: www.votealexissolis.com · Instagram: @ms.lexisolis · LinkedIn: Alexis Solis
The State of Women Institute · thestateofwomen.org · @thestateofwomen
‘Really? We Won?’ — What Nobel Laureate Claudia Goldin Means When She Says Women Won
Every time Claudia Goldin reveals the title of her ongoing research to a woman, she gets the same response. The work is called "Why Women Won," and almost without exception, the answer comes back: Really? We won?
It's a fair reaction. Open a newspaper. Look at the state of maternal mortality in the United States, the only wealthy country where it has been rising. Think about paid parental leave, which the U.S. remains nearly alone among developed nations in not guaranteeing. Think about the cost of childcare. Think about the gender pay gap that refuses to close.
And still, she means it.
March 4, just days before International Women's Day, Goldin delivered "Why Women Won" as the NIH Director's Lecture at the National Institutes of Health, one of American science's most prestigious platforms. The full talk is available to watch on the NIH videocast platform. It is an hour well spent. Goldin is the Henry Lee Professor of Economics at Harvard University and the 2023 Nobel laureate in economics, the first woman ever to win that prize unshared. This month, the American Academy of Arts and Sciences named her the recipient of its 2026 Talcott Parsons Prize, awarded every few years for high-impact contributions across the social sciences.
What she has built over a career at Harvard is harder to summarize than a list of honors. It is something closer to an archive of the economic lives of American women across two centuries, assembled from sources that other researchers either overlooked or never thought to look for.
The Economist as Detective
Goldin has described herself, since childhood, as wanting to be a detective. The Nobel committee took her at her word: her official Nobel portrait depicts her with a magnifying glass, a Sherlock Holmes hat, and a Golden Retriever. She grew up in the Bronx, attended the Bronx High School of Science intending to study bacteriology, and was redirected entirely by an economics professor at Cornell who revealed that discovery was the whole point — that economics, done right, was another form of hunting for hidden truths.
She earned her doctorate at the University of Chicago, was denied tenure at Princeton (economic history, she has noted, wasn't valued there at the time), and arrived at Harvard in 1990. Her method is to read the present through the past. In 1981, she went to the National Archives and, with a researcher's permission, rifled through boxes of Women's Bureau surveys that had sat largely untouched for decades — work histories, marriage bar records, wage data. She found surveys from 1939 in which managers, before any anti-discrimination legislation existed, answered candidly whether their firms fired women when they married. Many did. "The forms tell stories, and I listen," she has written in her Nobel biographical essay, "The Economist as Detective."
Her books include Understanding the Gender Gap: An Economic History of American Women (1990) and Career & Family: Women's Century-Long Journey Toward Equity (2021), the latter translated into fifteen languages. In announcing her as this year's Parsons Prize honoree, the Academy highlighted her pioneering work on women as economic operators — women as people who make decisions, build careers, navigate markets, and control, or don't control, their own money, their own names, their own futures.
A World Not So Long Ago
"Why Women Won" opens with a reminder that should not need to be a reminder.
Within living memory, women were routinely and legally fired when they married or became pregnant. They could not always get a credit card in their own name, or legally choose their own name. Decades after winning the right to vote, women had not yet obtained equal legal rights in the workplace, in marriage, in family law, in Social Security, in criminal justice, or in credit markets. The word "discrimination," as applied to women's treatment at work, was barely in common use — because the concept was not yet widely recognized as applicable to women at all.
Goldin has compiled a chronology of 155 critical moments in U.S. women's rights history, spanning 1908 to 2023, sorted into four categories: workplace rights, economic and social rights, political rights, and rights over their own bodies. Of those 155 moments, 45 percent occurred in a single decade, between 1963 and 1973. The Equal Pay Act. Title VII of the Civil Rights Act, with the word "sex" added almost accidentally by a congressman who initially intended it as a kill shot against the entire bill. Title IX. The Equal Credit Opportunity Act. No-fault divorce laws spreading across the states. And in January 1973, Roe v. Wade — which Goldin describes in her research as a success none of its supporters had predicted, an unexpected gift to the women's movement.
The word "fortuitous" appears more than once in her analysis of this period, and she means it precisely. The Civil Rights and anti-war movements changed everything. Women saw that their issues were not being discussed, and they learned to organize and leverage their power as an increasingly important voting bloc. But the legislative cascade that followed was not inevitable. It was contingent, fought-for, and at several critical moments, lucky.
"I find it impossible to imagine my world would be the same had women's rights remained as they were when I entered this institution as an undergraduate," Goldin told the Cornell Daily Sun. She received her undergraduate degree from Cornell in 1967, in the years just before that cascade began.
The Pill, the Paycheck, and the Body
Among Goldin's most celebrated findings is the research she conducted with Harvard colleague and husband Lawrence Katz on oral contraceptives and women's economic outcomes. The pill was approved by the FDA in 1960, initially for married women only. State laws restricting access for unmarried women were common. In her Nobel biographical essay, Goldin described the reality for young women of her own Cornell generation: putting fake rings on their fingers to convince doctors they were married, in order to get a prescription.
The state laws changed at different times and in ways that were effectively random, and Goldin and Katz used that variation as a natural experiment to measure the pill's causal effect on women's professional lives. Access to the pill increased the age at which women first married, which meant women could invest more heavily in professional training before family obligations arrived. Women made up 10 percent of first-year law students in 1970. By 1980, they made up 36 percent — a shift that coincided almost exactly with the cohort that came of age with access to contraception. Women with access to the pill experienced narrower wage gaps than those without.
Goldin's own chronology of women's rights, which runs through 2023, names Dobbs v. Jackson Women's Health Organization — the 2022 Supreme Court decision that overruled Roe v. Wade — explicitly among the history's documented "downs."
Why the Gap Persists
Legal rights, even sweeping ones, did not close the gender pay gap. In her American Economic Association presidential address, Goldin argued that the primary driver of the remaining gap was not discrimination in the traditional sense. It was the structure of work itself.
She describes certain positions as "greedy jobs" — those that disproportionately reward long hours, constant availability, and relentless schedule flexibility. These jobs pay substantially more than positions with predictable hours. And because women continue to carry a disproportionate share of caregiving at home, they disproportionately step back from these positions when family obligations arrive. The pay gap that results is not mainly employers paying women less for identical work. It is couples making rational choices inside a system that penalizes the person who takes the 3 p.m. call from school.
Why Women Are Divided
"Why Women Won" does not stop at the victories. It takes on the harder question in Goldin's research: why are women so divided about the very rights that would benefit them?
Her answer, drawn from decades of polling data including Gallup surveys, the General Social Survey, and the American National Election Studies, is that divisions among women by marital status, employment, religion, and region have consistently been greater than the divisions between men and women as a whole. This was true before the women's movement peaked in the early 1970s, and it deepened as the movement succeeded. Each legislative win caused some women to feel their goals were met and step back from organizing, leaving the remaining voices to appear increasingly radical to outsiders. The traditionalist and anti-feminist movement that organized in the early 1970s — initially around opposition to the ERA, then galvanized further by Roe v. Wade — remains, as Goldin writes in her NBER paper, a potent force in American politics today.
The word "feminist" became a casualty along the way. Even when large majorities of Americans supported expanding women's rights, Goldin's polling data shows that almost no one in any era would apply that word to themselves. The demonization of the term was not accidental. It was one of the most effective tools the opposition had, and its impact is still measurable in the data.
Rights Without Infrastructure
The comparison with peer nations sits near the center of Goldin's argument. The United States led other wealthy countries in granting women formal legal rights. It has lagged most of them, significantly, in providing the practical support that makes those rights livable. The U.S. led in terms of codifying rights but continues to lag in support for maternity and parental leave and childcare, compared to other industrialized countries.
American women won access to law school, medical school, credit, and equal employment protection. What they did not win — what women in Germany, Sweden, Canada, and Japan gained alongside or in place of formal legal equality — was the infrastructure: paid leave, subsidized childcare, labor structures that don't demand a binary choice between professional ambition and having a family. Goldin's research suggests this was not simply a political failure of timing. The traditionalist movement specifically and effectively stymied progress on paid family leave and subsidized childcare. Those consequences are still being lived.
The Long View
When asked whether she is pessimistic about the future of women, Goldin points to the smiley face she puts beside the word "won" in her talk title. "People often ask me if I'm pessimistic about the future of women," she has said. "Which is why I put that happy face on."
The optimism is archival, not sentimental. Goldin has spent her career with the actual data of actual women's lives across more than a century, assembled document by document from archives and survey boxes and old city directories. From that vantage point, what the record shows is plain: things were worse before. Specifically, documentably, legally worse. Not so long ago.
The history she has built includes Dobbs. It includes the defeat of the Equal Rights Amendment. It includes organized opposition that stalled paid family leave for a generation. The arc she traces is not smooth. It is a record of what was won, by whom, through what combination of strategy and luck and sustained pressure, and what it cost when parts of it slipped back.
That is, finally, the point of the title. Not a declaration that the work is done. A documented account of how much has already been accomplished — and a foundation from which the next chapter can be written with some knowledge of what the earlier ones actually contained.
Dr. Claudia Goldin's research, including the NBER working paper "Why Women Won," is publicly available at nber.org. Her book Career & Family: Women's Century-Long Journey Toward Equity is available wherever books are sold. The American Academy of Arts and Sciences will formally present her with the 2026 Talcott Parsons Prize on April 16.
Photo by Editing1088, licensed under CC BY-SA 4.0. Source: https://creativecommons.org/licenses/by-sa/4.0/
Sources
"Why Women Won" — NIH Director's Lecture, March 4, 2026. Event page and full videocasthttps://oir.nih.gov/wals/2025-2026/why-women-won
"Why Women Won" — NIH Videocast (full lecture, free to watch)https://videocast.nih.gov/watch/924bddcc-0174-11f1-9f14-124f0a52e769
"Why Women Won" — NBER Working Paper No. 31762, Claudia Goldin (October 2023, revised September 2025)https://www.nber.org/papers/w31762
"Claudia Goldin Wins Talcott Parsons Prize for Social Scientists" — Harvard Gazette, March 5, 2026https://news.harvard.edu/gazette/story/newsplus/claudia-goldin-wins-talcott-parsons-prize-for-social-scientists/
"The Economist as Detective" — Claudia Goldin Nobel Biographical Essay, NobelPrize.orghttps://www.nobelprize.org/prizes/economic-sciences/2023/goldin/biographical/
Career & Family: Women's Century-Long Journey Toward Equity — Claudia Goldin, Princeton University Press (2021)https://press.princeton.edu/books/hardcover/9780691201788/career-and-family
Understanding the Gender Gap: An Economic History of American Women — Claudia Goldin, Oxford University Press (1990)https://global.oup.com/academic/product/understanding-the-gender-gap-9780195072709
"The Power of the Pill: Oral Contraceptives and Women's Career and Marriage Decisions" — Claudia Goldin and Lawrence F. Katz, Journal of Political Economy (2002)https://www.journals.uchicago.edu/doi/10.1086/340778
Claudia Goldin — full publications list, Harvard Universityhttps://scholar.harvard.edu/goldin/publications
Science Made Simple: This Is Not an Awareness Campaign. It Is an Elimination Strategy.
EVIDENCE TO ACTION | Science Made Simple Special Edition | International HPV Awareness Day | March 4, 2026
By Dr. Odessa Lacsina, Executive Director, The State of Women Institute
I am writing this from Guyana.
Being here — meeting women for whom cervical cancer screening will be accessible for the very first time — makes this research personal in a way that no amount of reading could. The science is ready. The will is building. And the work is happening right now, in real time, in communities that have waited long enough.
Every March 4, the world observes International HPV Awareness Day. Most campaigns ask us to raise awareness. We are asking something different: to raise our expectations.
Cervical cancer is preventable. We have the tools — HPV vaccination and organized screening. What we have lacked is the will to deploy them together, equitably, and at scale. A landmark study published in Nature Communications changes the conversation — not from ignorance to awareness, but from awareness to infrastructure.
This edition of Science Made Simple breaks down what the research shows, what it means for you, and what it demands from our systems. Because the science is no longer the barrier.
The Study That Changes What Elimination Means
In 2021, researchers in Stockholm did something straightforward that turned out to be quietly radical. Led by Arroyo Mühr and colleagues, the team sent an invitation to every woman in the region born between 1994 and 1999 — all 89,547 of them — and made them an offer: come in once, get your HPV vaccine and your cervical screening done at the same visit, and go home.
No separate appointments. No choosing one or the other. Both, together, in a single visit.
The scientific term for this approach is a concomitant strategy — doing two interventions simultaneously rather than sequentially. But the underlying question was simpler than the terminology: is doing both at once actually faster at getting us to elimination than doing either one alone?
Of the nearly 90,000 women invited, 26,125 — just under 30 percent — enrolled between 2021 and 2022. What the researchers found when they modeled the data was striking.
In the cohorts that had already been offered the HPV vaccine years earlier, two of the most dangerous strains — HPV16 and HPV18 — had already declined significantly. That was vaccination doing its job over time. But vaccination has an inherent limitation: it takes decades for a vaccinated generation to age through the window of risk. In the meantime, HPV keeps circulating among people who were never vaccinated.
Screening addresses a different part of the problem. It doesn't prevent infection — but it catches what's already there, identifying abnormal cells before they can become cancer. The catch is that screening has to be repeated, because it can't stop new infections from occurring.
Put the two together, though, and something different happens. The model predicted a 62 to 64 percent reduction in high-risk HPV infections within just three years of implementing the combined strategy. Not decades. Three years. The researchers described it as a compounding public health effect — each intervention amplifying the other in ways that neither could achieve alone, producing what the study called near-complete protection when both were combined.
The conclusion Arroyo Mühr and her colleagues drew was direct:
*"Concomitant HPV vaccination and HPV screening appears to be a realistic option for faster cervical cancer elimination."*¹
Not aspirational. Not theoretical. Realistic — with the right infrastructure behind it.
Science Made Simple: What This Means in Plain Language
The old message was: Get vaccinated.
That message has saved lives. HPV vaccines are among the most effective cancer prevention tools ever developed. But vaccination alone has a time problem — it takes decades for a vaccinated generation to grow up, and in the meantime, HPV keeps spreading among adults who were never vaccinated.
The new message is: Vaccinate AND screen. At the same time. For everyone.
Screening has something vaccination doesn't: speed. Once a woman is screened, the benefit is immediate — abnormal cells can be found and treated before they become cancer. Combined with vaccination, you get short-term protection from screening and long-term elimination from vaccination. The two tools work differently, and that's precisely why they work better together.
Why Together Is Not Just Better — It's Transformational
Think of it this way:
Vaccination stops future infections from taking hold.
Screening catches current infections before they become cancer.
When you do both — you stop what's coming AND address what's already here.
That is how you move from management to elimination.
Why Black and Brown Women Need This Most
The benefits of this combined strategy are not distributed equally — and neither are the harms when systems fail to implement it.
In the United States, Black women are significantly more likely to be diagnosed with cervical cancer at advanced stages and to die from the disease — not because of biology, but because of systemic disparities in access to both vaccination and screening.
According to the CDC, only 38% of Black women have received the HPV vaccine, compared to 48% of white women.² Hispanic women face even greater barriers, with many reporting they didn't know they needed screening at all. These are not knowledge failures. They are infrastructure failures.
What the disparity looks like:
Black women are twice as likely to die from cervical cancer as white women²
Hispanic women have the highest cervical cancer incidence rate of any racial or ethnic group in the U.S.²
Women without health insurance report 7x more difficulty accessing cervical cancer screening²
Knowledge gaps about HPV and its link to cancer are significantly higher among Black and Hispanic populations²
The combined vaccination and screening strategy is especially critical in underserved communities — where neither tool alone has been delivered consistently
Six Things Every Woman Should Know
1. You can get vaccinated as an adult. The HPV vaccine is approved through age 45. If you were never vaccinated, or didn't complete the series, talk to your provider. It is not too late.
2. Vaccination and screening are not either/or. Getting the vaccine does not mean you can skip your Pap smear or HPV test. This research confirms that doing both is significantly more protective than either alone.¹
3. Self-collection is now an option. In many settings — including the Guyana HPV Elimination Initiative — women can collect their own cervical sample for HPV testing. This removes one of the biggest barriers to screening: access to a clinic.
4. Your birth year matters. Women born before widespread vaccination was available — particularly those born before the late 1990s — may not have vaccine protection, and are the exact population this study targets for the concomitant strategy.¹
5. Ask your provider specifically. Don't just ask if you are "up to date." Ask: Have I been tested for high-risk HPV strains? Have I been offered vaccination? What screening interval is right for my age and history?
6. This is about systems, not just personal choices. The most important thing you can do is demand that your healthcare system, your employer, and your elected officials invest in making both vaccination and screening universally accessible — not just available to those who can afford it.
"The science is no longer the barrier. This initiative is how we build effective systems." — Dr. Odessa Lacsina, Executive Director, The State of Women Institute
Take Action: Three Steps This Week
Step 1 — Know Your Status
Call your provider and ask: When was my last HPV screening? Have I been tested for high-risk HPV strains?
If you haven't been screened in the past 3–5 years, schedule an appointment this week
Ask about self-collection options if a clinic visit is a barrier for you
Step 2 — Protect Yourself and the People You Love
Share this post with one woman in your life who may not have been vaccinated or screened recently
If you have a daughter, niece, or young woman in your community — make sure she knows the HPV vaccine is recommended starting at age 9
The vaccine works best before exposure, but it has benefit at any age through 45
Step 3 — Demand Infrastructure
Contact your local health department or elected representative and ask what cervical cancer screening programs exist in your community
Support organizations — including The State of Women — that are building the delivery systems this research calls for
Follow the Guyana HPV Elimination Initiative for real-time updates on what elimination looks like in practice
Cervical cancer is preventable. Elimination is possible: Where women's voices build the systems that sustain their health.
Evidence to Action | The State of Women Institute | thestateofwomen.org
Sources
¹ Arroyo Mühr LS, Gini A, Yilmaz E, Hassan SS, et al. "Concomitant human papillomavirus (HPV) vaccination and screening for elimination of HPV and cervical cancer." Nature Communications, Vol. 15, Article 3679, May 1, 2024. https://doi.org/10.1038/s41467-024-47909-x
² Centers for Disease Control and Prevention. HPV Vaccination Coverage and Cervical Cancer Disparities Data. https://www.cdc.gov/hpv
Patient Recognition Week: Why Women Deserve to Be Believed the First Time
What does it mean to truly recognize a woman as a patient? It means believing her pain the first time she describes it, and treating her as the expert on her own body. During National Patient Recognition Week, that shift—from doubting to trusting, from brushing off to leaning in—may be one of the most powerful ways healthcare can honor women’s lives.
Checking in on Patients
National Patient Recognition Week, observed February 1–7, was created to spotlight patient satisfaction, empathy, and human-centered care in clinics and hospitals across the United States. Healthcare organizations are encouraged to listen more carefully, encourage feedback, and recommit to compassionate treatment and respect for every person who walks through their doors.
In 2026, the theme emphasizes hearing and respecting patients’ voices and weaving their lived experience into care decisions. Some organizations mark the week with social media campaigns, appreciation notes, or small events; others use it to review communication practices and experience surveys with an eye toward real improvement. The week strives to ask a basic question: Do patients feel like human beings whose stories matter, not just the next name on a schedule?
For many women, the honest answer is still “not always.”
When Women’s Pain Isn’t Believed
Decades of research show that women’s pain is more likely than men’s to be minimized, psychologized, or misattributed, even when symptoms are similar. Studies and clinical reviews have documented patterns where women describing pain are more often told their symptoms are due to stress or emotions, while men with comparable complaints are offered diagnostic tests or stronger pain relief. Old stereotypes about women being “dramatic” or “hysterical” may be out of fashion in name, but they linger in how some symptoms are interpreted.
The stakes are high. Chronic pain conditions that disproportionately affect women—endometriosis, pelvic pain, interstitial cystitis, vulvodynia, certain autoimmune conditions—can take years to diagnose. In that time, a woman may see multiple providers, repeat her stories over and over, and still feel like no one appreciates the intensity of her symptoms, reality of her experience, or depth of her concerns. When a clinician finally listens and takes their words seriously, it can change the course of a patient’s care: Treatment plans are adjusted, imaging ordered, referrals made, and women stop hearing that it’s “all in your head.”
Here, “recognition” isn’t a slogan or a card on a bulletin board. It’s what happens when a provider hears a woman describe her pain and automatically treats that account as credible and important. It starts with belief rather than skepticism.
When Women Are Missing From the Data
Bias doesn’t only show up in the exam room. It’s also baked into the research that shapes standards of care. For years, clinical trials often under-enrolled women or failed to analyze sex-specific data, treating male bodies as the norm and female bodies as a variation on that norm. Policies have improved, but major gaps remain, especially for conditions that primarily or exclusively affect women.
Pain management is one example. Reviews of the field highlight how stereotypes, unequal study designs, and a lack of high-quality, gender-aware research all feed into misdiagnosis and undertreatment of women’s pain. When diseases, devices, and drugs are studied in populations that don’t reflect women’s bodies and lives, the message is clear: women’s health isn’t driving the agenda.
If Patient Recognition Week is about honoring the patient voice, then for women that has to include research that reflects their realities. Recognition isn’t only “We’ll listen during your appointment.” It also means, “We’re designing studies, treatments, and protocols with you in mind.”
Heart Disease: The Risk Women Don’t Expect
Heart disease shows how belief and representation in the data both matter. Cardiovascular disease is the leading cause of death in women worldwide and in the United States, responsible for an estimated 30% of deaths among women—more than all forms of cancer combined. Yet many women still don’t recognize heart disease as their top health threat, and gender bias has contributed to under-diagnosis and under-treatment.
Symptoms can look different in women. Instead of the classic “crushing chest pain” image that’s often associated with men, women may experience severe fatigue, shortness of breath, nausea, lightheadedness, or pain in the back, jaw, or neck. Those complaints are easy to dismiss as anxiety, indigestion, or stress—by women themselves and sometimes by their providers. Time is lost, and so is trust.
Patient recognition here means clinicians are trained to look for sex-specific patterns, take these symptoms seriously, and treat a woman’s sense that “something isn’t right” as a critical piece of information. Public messaging matters too: awareness campaigns that speak directly to women’s risks and symptoms help women know when to seek care.
The Hidden Cost of Asking Women to “Advocate Harder”
Women are often told to advocate for themselves in medical settings: ask more questions, bring a list, speak up if something feels off. Those tools can help, and practical strategies like symptom logs, written questions, or bringing a friend do make it easier to get clear answers. But when the system doesn’t change, “self-advocacy” can quietly shift responsibility onto women for fixing the bias they face.
Experts in women’s health and pain management note that many women brace for their symptoms to be doubted, especially when they involve reproductive health, pelvic pain, or conditions that mainly affect women. That constant vigilance comes at a cost. It’s draining to walk into every appointment assuming you’ll have to prove your own pain. It’s wearing to tell the same story again and again, hoping that this time someone will take it seriously.
Patient Recognition Week gives clinics and health systems a chance to turn away from that pattern. Instead of asking women to fight harder, they can ask what it would look like to listen better and change structures that make women feel unheard in the first place.
What True Recognition Could Look Like
If healthcare decided to use this week to genuinely recognize women as experts in their own bodies, a few practical steps could make a real difference.
Listening sessions with women patients. Clinics can host small listening circles or online surveys inviting women from different backgrounds to share moments when they felt heard—and when they didn’t. Themes from those conversations can inform staff training, appointment workflows, and communication policies.
Gender-aware training on pain and symptoms. Ongoing education can help providers spot the ways gender bias creeps into pain management and diagnosis, from assuming women exaggerate symptoms to overlooking heart disease when complaints don’t fit the “classic” pattern. Small adjustments—a different follow-up question, a lower threshold for testing—can prevent years of missed or delayed care.
Clear protocols for women’s health conditions. Building or updating clinical pathways for endometriosis, chronic pelvic pain, and other women’s health issues signals that the clinic expects these conditions, takes them seriously, and has a plan. That can make women feel less like outliers and more like patients whose needs were anticipated.
Better feedback loops. Instead of relying only on generic satisfaction surveys, organizations can ask women specific questions: “Did you feel listened to?” “Did your provider believe your description of your symptoms?” “Did you feel safe talking about pain or sensitive concerns?” Responses can drive concrete changes in scheduling, staffing, or communication tools.
Centering women in public messaging. During heart health campaigns in February or Patient Recognition Week posts, including women-focused risk information and symptom lists makes messages more accurate and more useful. When women see their experiences described, they’re more likely to recognize warning signs and seek care.
None of this replaces the need for skilled clinicians, strong science, or evidence-based treatments. Medical expertise and high-quality research are essential foundations. The point is to pair that expertise with the knowledge women have about their own bodies and lives, rather than treating those experiences as secondary.
For Women Reading This: You Deserve to Be Believed
If you’re a woman who’s been told “it’s probably nothing” when it didn’t feel that way, you’re not alone. If you’ve had a provider wave off your pain or walked out of an appointment thinking, “They didn’t really hear me,” that experience is unfortunately common—and it’s part of a larger pattern, not a personal shortcoming.
A few simple steps can make medical visits feel more manageable:
Write down the basics ahead of time. Note your main symptoms, when they started, what makes them better or worse, and what you’re most worried about. You don’t need medical language; your own words are enough.
Bring someone you trust. A friend or family member can help you remember details, take notes, or speak up if you get flustered.
Keep one or two key questions in mind. Questions like “What else could this be?” or “If I were your sister, what would you recommend next?” can open the door to clearer explanations and more thoughtful care.
These strategies can’t fix systemic bias on their own, and they shouldn’t have to. But they can give you a bit more steadiness in the room while broader changes take shape.
A Week to Ask Better Questions
National Patient Recognition Week often shows up in warm social media posts and cheerful graphics celebrating patients—and that kindness matters. It’s also a natural point in the calendar for clinics and health systems to ask harder questions: Do women feel believed here? Do they feel their pain counts? Do they see themselves reflected in our research, our protocols, and our public messaging?
Recognizing women as patients means treating them as central decision-makers and credible narrators of their own health, not passive recipients of care. It means acknowledging the research gaps and diagnostic patterns that have left women under-diagnosed and under-treated, and then doing something about them. It means understanding that the best care comes from combining medical knowledge with the lived experience women bring into the exam room.
If you work in healthcare, this week is a chance to talk with women in your practice, examine where bias might be showing up, and pick at least one concrete change that makes it easier for women to be believed the first time they speak. If you’re a patient, it’s a reminder that your symptoms are real, your perspective matters, and you have every right to care that treats you as the expert on your own body.
That’s the kind of recognition women’s health has been missing—and the kind that can spare years of suffering, and sometimes, save lives.
Sources
“The Girl Who Cried Pain: A Bias Against Women in the Treatment of Pain”
https://pubmed.ncbi.nlm.nih.gov/11521267/
American Medical Women's Association - Pain Management Review
https://amwa-doc.org/pain-management-reviewing-research-that-highlights-differences-in-pain-assessment-and-management-between-patients/
Cardiometabolic Health Alliance - Heart Disease as #1 Cause of Death for Women
https://www.cardiometabolichealth.org/heart-disease-remains-leading-cause-of-death-for-women-addressing-the-gender-bias-in-cardiovascular-care/
World Heart Federation - Women & CVD
https://world-heart-federation.org/what-we-do/women-cvd/
Holding Ground on Maternal Health: What Maternal Health Awareness Day Means in 2026
January 23 marks Maternal Health Awareness Day, an annual observance that confronts an uncomfortable truth: pregnancy and childbirth in the United States remain far more dangerous than they should be. For a country that spends more on healthcare per capita than any other developed nation, our maternal mortality rates tell a different story.
This year’s theme, “Holding Ground on Maternal Health,” chosen by American College of Obstetricians and Gynecologists, isn’t about celebrating motherhood or sharing feel-good statistics. It's about reckoning with the preventable deaths, the widening disparities, and the systemic failures that make bringing life into the world a matter of survival for too many women.
The Numbers Tell a Grim Story
The United States has the highest maternal mortality rate among developed nations. Maternal deaths surged dramatically from 658 in 2018 to a devastating peak of 1,205 in 2021—the highest in over 50 years. While COVID-19 played a significant role in that spike, the underlying crisis predates the pandemic.
The overall numbers have improved since 2021, dropping to 817 deaths in 2022 and 669 in 2023. But those improvements haven't been shared equally, and the racial disparities have actually worsened.
Black women face a maternal mortality rate of 50.3 deaths per 100,000 live births—more than three times higher than white women at 14.5 per 100,000. Hispanic women have a rate of 12.4 per 100,000, and Asian women 10.7 per 100,000.
What's especially troubling is that the gap has widened. In 2021 and 2022, Black women died at rates about 2.6 times higher than white women. By 2023, that disparity increased to 3.5 times higher. As the pandemic eased and overall maternal deaths declined, white and Hispanic women saw significant decreases, while rates for Black women remained essentially unchanged.
What makes these statistics even more troubling is that they're largely preventable. According to research from organizations like the CDC Foundation and March of Dimes, up to 80% of pregnancy-related deaths could be avoided with timely intervention, proper screening, and continuity of care.
The problem isn't a lack of medical knowledge. We know what causes maternal deaths. We know how to prevent them. What we're missing is the infrastructure, the prioritization, and often the will to make sure every pregnant person has access to the care they need.
Most Deaths Happen After Delivery
Here's something that surprises many people: the majority of maternal deaths don't occur during labor or delivery. They happen in the weeks and months after birth.
The postpartum period has long been treated as an afterthought in American healthcare. A single six-week check-up became the standard decades ago, and for many women, that's still all they get. But complications like blood clots, infections, uncontrolled high blood pressure, and mental health crises don't always show up on a predictable timeline.
Hemorrhage, hypertensive disorders like preeclampsia and eclampsia, cardiovascular conditions, infections, blood clots, and mental health emergencies including suicide are among the leading causes of maternal death. Many of these conditions can develop or worsen well after a woman leaves the hospital.
Despite this, insurance coverage for comprehensive postpartum care remains inconsistent. Many providers don't have systems in place to track patients after discharge or follow up when warning signs appear. Women are often left to self-monitor and self-advocate at a time when they're exhausted, overwhelmed, and adjusting to life with a newborn.
Maternity Care Deserts Are Expanding
If you live in a major city, it might be hard to imagine not having access to a hospital with a maternity ward. But for over 2 million women across the United States, that's reality. They live in counties with no hospital offering obstetric care, no birth center, and no OB-GYN.
Rural communities have been hit hardest. Since 2022, more than 100 hospitals across the United States have closed their obstetric units. Maternity wards across the South and Midwest have shuttered at alarming rates over the past decade, driven by financial pressures, staffing shortages, and consolidation of healthcare systems.
The economics are brutal: maternity units must operate 24/7, but reimbursement rates don't cover costs, especially for smaller community hospitals. Women are traveling hours to deliver their babies, sometimes delivering in emergency rooms that aren't equipped for childbirth.
The Maternal Health Workforce Crisis
The maternal health workforce is shrinking, and it's not just about hospital closures. Multiple factors are driving providers out of the field:
Nearly 30% of OB-GYNs report experiencing burnout, and 23% deal with both burnout and depression. Forty percent say their work-life balance has gotten worse over the past three years. The administrative burden—excessive paperwork, charting requirements, and bureaucratic tasks—compounds the stress of an already demanding specialty.
But burnout isn't the only problem. There simply aren't enough training spots to meet demand. In the 2025 Match, 2,151 applicants competed for only 1,587 OB-GYN residency positions, leaving 564 qualified applicants without a spot. Even if every position were filled, we still wouldn't have enough OB-GYNs, midwives, and labor and delivery nurses to safely staff maternity units across the country.
The shortage is most acute in underserved and rural communities, where it's harder to recruit providers. And the underlying issue goes deeper: the care of women and children has been chronically undervalued in the broader healthcare system—underfunded in reimbursement rates and overlooked in policy priorities.
This creates a dangerous gap. When care is far away or providers are stretched too thin, women miss appointments. Complications go undetected. Risk factors pile up. And when something goes wrong, there's no safety net close by.
Mental Health Is Part of Maternal Health
Postpartum depression and anxiety affect about 1 in 7 new mothers, but many cases go undiagnosed or untreated. Postpartum psychosis is rarer but can be life-threatening when it occurs.
Suicide and overdose are among the leading causes of death in the first year after giving birth. Yet mental health screening during pregnancy and the postpartum period remains inconsistent across the country. Access to treatment is even more fragmented.
There's still stigma around admitting you're struggling after having a baby. New mothers are expected to be glowing, grateful, and bonded to their infants. When reality doesn't match that picture, many women suffer in silence rather than ask for help.
Supporting maternal health means recognizing that emotional and psychological well-being are just as critical as physical recovery. Screening needs to happen routinely, not as an afterthought. Treatment needs to be accessible, affordable, and free of judgment.
How Women Are Treated Matters
One of the most well-documented factors in maternal mortality is the quality of care women receive—and specifically, whether they're listened to and believed when they raise concerns.
Study after study has shown that Black and Indigenous women report being dismissed, ignored, or disbelieved when they talk about pain or symptoms during pregnancy and after birth. This isn't anecdotal. It's measurable, it's pervasive, and it's deadly.
Even high-profile cases have highlighted this issue. Serena Williams, one of the greatest athletes in the world, had to fight to get her medical team to take her concerns seriously after giving birth, despite her history of blood clots. If someone with her resources and platform faces that kind of dismissal, what happens to women without those advantages?
Culturally competent, trauma-informed, patient-centered care isn't optional. It's essential. Women need to be treated with dignity and respect, especially when they're at their most vulnerable. Their lived experiences and knowledge of their own bodies should be valued, not questioned.
What You Can Actually Do
Maternal Health Awareness Day isn't just about raising awareness—it's about turning that awareness into action.
Advocate for policy change. Support Medicaid expansion, paid family leave, and federal and state legislation that funds maternal health programs and addresses racial disparities. The Black Maternal Health Momnibus Act represents comprehensive legislation specifically designed to tackle maternal health inequities. Contact your representatives. Make your voice heard.
Support community organizations. Many grassroots groups are filling gaps in the healthcare system by providing doula services, prenatal education, lactation support, and postpartum care—especially in underserved communities. Organizations like the National Birth Equity Collaborative, Black Mamas Matter Alliance, March of Dimes, and local community health centers often operate on limited budgets and rely on donations and volunteers.
Educate yourself and others. Share accurate information about maternal health. Challenge myths. Talk about the realities of pregnancy and postpartum recovery, not just the sanitized version that gets posted on social media. Reliable sources include the American College of Obstetricians and Gynecologists (ACOG), the CDC Foundation's Hear Her Campaign, and organizations centered on birth equity.
Amplify lived experiences. Listen to mothers, especially those from marginalized communities. Their stories reveal what data alone cannot. They show where systems fail, where support is lacking, and where change is desperately needed.
Stories Behind the Statistics
Behind every maternal mortality statistic is a person. A mother who didn't come home from the hospital. A family forever changed by a loss that should never have happened. A survivor who fought through complications that proper care could have prevented.
We need to hear from OB-GYNs who are tracking patterns in their patients and seeing firsthand where the system breaks down. From midwives expanding access in rural areas where hospitals have closed. From doulas supporting families through traumatic births. From mothers who've had to fight to be believed when they knew something was wrong.
These stories don't just humanize the crisis. They show us where change is possible and who's already doing the work to make it happen.
Holding the Ground
This Maternal Health Awareness Day, we're holding ground.
We're not backing down on the demand for equitable, accessible, respectful care for every pregnant and postpartum person in this country. We're not accepting maternal mortality rates that belong in the last century. We're not pretending that awareness alone will solve this crisis.
Mothers deserve better. Families deserve better. Communities deserve better.
And we have the knowledge, the tools, and the resources to make it happen. What we need now is the commitment to follow through.
Resources:

Science Made Simple: Your Brain Has Two Ages
EVIDENCE TO ACTION | Science Made Simple The State of Women Institute
By Dr. Odessa Lacsina, Executive Director, The State of Women Institute
Your driver's license says you're 55. But your brain? It could be living its best 47-year-old life — or, less encouragingly, acting more like it's 63.
New research out of the University of Florida reveals something genuinely surprising: your brain has two ages. The first is your chronological age — how many birthdays you've had. The second is your brain age — how your brain actually looks on an MRI scan. And here's what makes this research worth paying attention to: you get to influence which one matters more.
The Eight-Year Finding
Scientists at the University of Florida tracked 128 adults over two years and found that people with the healthiest lifestyle habits had brains that appeared up to eight years younger than their chronological age — and that their brains also aged more slowly over time, meaning the benefits kept accumulating.
Eight years. That is not a rounding error. That is a measurable, structural difference in how a brain looks on a scan, driven not by medication or medical intervention, but by daily habits.
Lead researcher Dr. Jared Tanner and his team, publishing in Brain Communications in December 2025, identified seven specific habits associated with younger-looking brains. None of them are exotic. All of them are within reach.¹
The Seven Habits
Quality sleep — not just time in bed, but actual restorative sleep
Optimism — which, the research suggests, can be practiced and cultivated
Social support — having people you can genuinely lean on
Stress management — developing the capacity to handle life's inevitable chaos
Healthy waist circumference — maintaining weight in a healthy range
No tobacco use
Positive mindset — focusing on what you can influence and control
Each habit adds another layer of protection. Critically, they work together — the benefits compound rather than simply adding up.
Why This Matters — Especially for Women
An older-looking brain is more vulnerable to memory decline, dementia, and Alzheimer's disease. And women are already at higher risk for Alzheimer's than men — making research like this particularly urgent, and particularly relevant to the health equity work at The State of Women Institute.
But here is what this research makes clear: we are not without agency. We have tools. The daily choices that shape brain health are not reserved for people with access to expensive interventions. They are, for most women, already within reach — and the evidence now tells us they matter more than we may have realized.
It's Never Too Late
One of the most important findings in this study: even people living with chronic pain — who typically show accelerated brain aging — saw protective benefits from healthy habits. The biology is not fixed. The brain responds.
Lifestyle is medicine. Your daily choices matter — not someday, but now. And you don't need to be perfect. Every small improvement counts, and the research suggests those improvements stack.
The Bottom Line
Your brain age is not set in stone. It is moldable, changeable, and responsive to the way you live. Sleep well. Stay hopeful. Stay connected. Find ways to manage stress that actually work for you.
The science is telling us something we can act on. That's the whole point of this series.
What is one habit you're going to focus on this week?
Source
¹ Tanner, J., et al. Brain Communications, December 2025. University of Florida.
Dr. Odessa Lacsina is the Executive Director of The State of Women Institute, a 501(c)(3) nonprofit working across three health equity pillars: Mental Health & Wellness, Maternal Health Equity, and Preventive Wellness.
To learn more or support women's health leadership, visitthestateofwomen.org or follow @thestateofwomen.

How Digital Violence Is Blocking Women’s Health in the Digital Age
Human Rights Day closes out the 16 Days of Activism, and this year’s theme—“UNiTE to End Digital Violence against All Women and Girls”—lands right in the middle of how women get health care today. More and more appointments, test results, birth control consults, and mental health check-ins happen through screens, apps, and portals—and digital violence is quietly pushing women away from those tools.
This isn’t just about “being safer online.” It’s about whether women and girls feel safe enough to reach for the care they need.
1. Digital violence is changing how women seek care
When a woman has been stalked, doxxed, or threatened online, opening a health portal or a telehealth app can feel risky, even if she trusts her provider. Fear that messages, photos, or location data could be leaked or weaponized can make her cancel appointments, avoid online booking systems, or stick to walk-in clinics instead of consistent care.
For survivors of digital violence, every notification can feel like a potential new attack. That kind of fear doesn’t just live in the mind; it can lead to missed screenings, delayed follow-ups, and untreated conditions because the digital doorway to care doesn’t feel safe.
2. Sexual and reproductive health care is especially vulnerable
Sexual and reproductive health information is already highly sensitive. Add digital violence, and many women start to worry that their search history, period tracking, telehealth abortion consults, or STI testing reminders could be exposed or used against them.
Partners or family members who monitor devices, demand passwords, or “check up” on messages can make it nearly impossible for women and girls to privately access contraception, abortion care, or information about consent and healthy relationships. That’s not a small inconvenience; it can change whether someone can plan a pregnancy, leave an abusive situation, or manage an infection in time.
3. The gender digital divide is also a health divide
In many places, women have less access to phones, data, and private internet—even as health systems move more services online. When a woman relies on a shared phone, a public computer, or a device controlled by a partner, she’s more exposed to digital abuse and has fewer safe ways to use digital health tools.
That means reminders, lab results, mental health chats, and contraceptive counseling may all run through channels where someone else can see or intercept them. The result is a double hit: greater risk of digital harassment and fewer safe, private options for getting care or accurate health information.
4. Privacy and data protection are now core health issues
Digital health tools collect all kinds of information: symptoms, sexual history, mental health notes, location, even details about pregnancy or abortion. When women hear stories about data breaches, tracking, or apps sharing sensitive details without clear consent, they may decide it’s safer not to use those tools at all.
That loss of trust can be its own kind of harm. Some women stop using mental health apps, delete period trackers, or avoid signing up for online portals, even when those tools could help them manage chronic conditions or stay on top of screenings. On Human Rights Day, it’s worth saying plainly: protecting women’s health data, and making sure it can’t be used to target or shame them, is part of the right to health in a digital world.
5. Digital trauma can follow women into the clinic
For women who have faced image-based abuse, online sexual harassment, or doxxing, opening a health app or logging into a telehealth visit can bring up memories of earlier violations. That “technology-related trauma” can make it hard to answer sensitive questions honestly, turn on a camera, or trust a message system—even with a kind provider on the other side.
This can be especially intense for people seeking abortion care, contraception, STI treatment, or mental health support after sexual violence. If a digital tool feels even a little unsafe or confusing, many survivors will simply drop out of care, or postpone it until things are more serious—adding to both physical and emotional strain.
6. Health workers need to see digital safety as part of care
Doctors, nurses, midwives, school health staff, and counselors are on the front lines of women’s health in this digital moment. When a woman seems hesitant about telehealth, avoids using the portal, or misses online follow-ups, it might not be “non-compliance”—it might be fear of digital surveillance, harassment, or leaks.
Simple questions like “Do you feel safe using your phone for health messages?” or “Is there anyone else who can see your health app or texts?” can open the door to better support. Providers can help women think through safer options—like using code words, turning off certain notifications, or scheduling in-person visits—so digital tools support health instead of becoming another source of harm.
7. The right to health includes safe digital spaces
Human Rights Day is about the promise that everyone has the right to the highest attainable standard of physical and mental health. In 2025, that promise has to include the right to use digital health tools—telehealth, apps, portals, messaging—without fear of violence, harassment, or misuse of deeply personal information.
Ending digital violence against women and girls isn’t only about stopping abuse on social media. It’s also about making sure women can check their lab results, message a doctor, manage a chronic condition, or access sexual and reproductive health care without wondering who might be watching or waiting to hurt them. When digital spaces are safer, women’s access to care expands, their mental and physical health improve, and the right to health becomes a little more real—on every screen, in every clinic, for every woman and girl.

16 Days of Activism: Why Digital Violence Against Women Demands Our Attention

Image: UN Women
Every ten minutes last year, a woman or girl was intentionally killed by a partner or family member. That's 137 women and girls every single day—around 50,000 over the course of 2024. These aren't abstract numbers. They're mothers, daughters, sisters, friends, colleagues—people with dreams and plans and voices that were silenced.
And increasingly, that violence starts long before physical harm occurs. It begins with a message. A threat. A stolen photo. A deepfake created by artificial intelligence. The latest UN report shows that technology-facilitated violence—like cyberstalking, coercive control, and image-based abuse—can be a risk factor that escalates offline and, in some cases, leads to femicide.
When screens become weapons
From November 25 through December 10, the world marks the 16 Days of Activism against Gender-Based Violence. This year's theme—"UNiTE to End Digital Violence against All Women and Girls"—addresses one of the fastest-growing forms of abuse women face.
What starts small on screens can quickly spiral into threats and violence in real life. Private photos get stolen and shared without consent. Lies spread within seconds. Women's locations are tracked. AI gets weaponized to create deepfakes designed to shame and silence.
The digital world should empower women and girls. Instead, for millions of them, it's become a minefield.
Who's affected most?
Digital violence targets women more than men, especially those with public or online visibility—activists, journalists, women in politics, human rights defenders, and young women. The impact hits even harder for women facing other forms of discrimination based on race, disability, gender identity, or sexual orientation.
Adolescent girls face some of the greatest risks. Their social and emotional development increasingly happens online, in spaces filled with gender bias and misogyny that can fuel lasting harm.
Consider the journalist who stops writing after death threats. The activist who deletes her accounts to protect her family. The girl who loses confidence before she's even found her voice.
Why the focus on digital violence now?
Several factors have converged to make digital violence a crisis that can't be ignored:
Weak regulation of the technology sector means there's often no legal recognition of digital violence in many countries. Tech platforms lack accountability. Misogynistic content in the so-called "manosphere" fuels abuse and spreads hate. When these toxic ideas go viral, they shape how entire generations see and treat women and girls.
AI has created new forms of abuse and amplified existing violence. There's a growing backlash against gender equality. The anonymity of perpetrators and cross-border nature of online abuse make it harder to get justice. Support systems for survivors remain limited.
And here's the thing: this is happening at a time when sweeping aid cuts are forcing women's organizations around the world to shut down or drastically scale back programs to end violence against women.
Progress and the road ahead
There's been some movement in the right direction. Thanks to years of advocacy by feminist and digital rights movements, major progress has been made. In 2024, the UN Statistical Commission called for the development of global methods to measure technology-facilitated gender-based violence. Regional bodies have acted too—from the African Union's Convention on Ending Violence against Women and Girls to the EU's Digital Services Act.
But we can't stop there.
#NoExcuse for violence
There is #NoExcuse for violence against women and girls. Nearly one in three women experience violence in their lifetime. For adolescent girls, the statistics are even more concerning: one in four is abused by their partners.
This year's 16 Days of Activism campaign has clear calls to action for different groups:
Governments need to pass and enforce laws that criminalize digital violence, protect personal information, and strengthen tech sector accountability.
Tech companies must ensure platform safety, remove harmful content quickly, enforce codes of conduct, and publish transparent reports about how they're addressing abuse.
Donors should invest in feminist organizations working to end violence against women and support digital rights advocates.
All of us can speak out, support survivors, and challenge harmful online norms. We can build critical thinking skills around online content, consent, and respectful relationships.
The bigger picture
The 16 Days of Activism runs from November 25 — the International Day for the Elimination of Violence Against Women — through December 10, which is International Human Rights Day. That connection isn't accidental.
Violence against women is a human rights issue. And as we approach the 30th anniversary of the Beijing Declaration and Platform for Action in 2025—one of the most important international agreements on women's rights—this campaign serves as a reminder that digital safety is central to gender equality.
Women belong online. Girls belong online. But they deserve to be there safely.
What comes next
Violence against women and girls can and must be prevented. This requires ending impunity by holding perpetrators accountable. It means adopting, implementing, and funding National Action Plans to end violence against women and girls. It calls for investing in prevention and women's rights organizations to ensure survivors have access to essential services.
The work isn't easy. But better to try, better to be on the right side of history, better to do the part that each of us can do.
Because there's #NoExcuse for violence. Not in person. Not online. Not anywhere.
The 16 Days of Activism against Gender-Based Violence runs from November 25 to December 10. Learn more about how to get involved at UN Women.
Follow the conversation using #NoExcuse and #16Days.
7 Healthcare Barriers Facing Hispanic Women

This Hispanic Heritage Month, we celebrate the strength, resilience, and contributions of Latina and Hispanic women across our communities. But along with honoring the past and future of Hispanic people is facing the reality that significant healthcare disparities affect millions of women and their families. These barriers aren't personal failings—they're systemic challenges that demand our attention and action.
These obstacles touch the lives of women and their families every day. Understanding them helps us build a healthcare system that works for everyone.
Economic Barriers That Create Impossible Choices
For many Latina women, healthcare becomes a luxury they can't afford. With higher rates of poverty and lower median incomes compared to other groups, medical bills can mean choosing between rent and a doctor's visit. Even with insurance, copays and deductibles can stretch budgets to the breaking point. When you're working multiple jobs just to keep your family afloat, taking time off for preventive care feels like a privilege few can afford.
The ripple effects extend beyond individual health. When mothers delay their own care due to cost, it affects entire families. Children miss check-ups, chronic conditions go unmanaged, and small health issues become major crises.
Language Barriers in a System That Doesn't Always Listen
Imagine trying to explain your symptoms, understand a diagnosis, or give informed consent for treatment in a language that isn't your first. For many Latina women, this is their reality every time they seek medical care. While federal law requires interpretation services, the quality and availability vary dramatically. Sometimes, family members—even children—end up translating sensitive medical information.
These language barriers affect more than communication. They impact trust, comprehension of treatment plans, and the ability to advocate for yourself in medical settings. When you can't fully express your concerns or understand your options, healthcare becomes something that happens to you rather than with you.
Insurance Gaps That Leave Too Many Behind
Despite improvements under the Affordable Care Act, Latina women remain more likely to be uninsured than their white counterparts. Mixed-status families face particular challenges, as immigration status can affect eligibility for public health programs. Some women avoid seeking care altogether, fearing that using public benefits might impact their family's immigration status.
Even when insurance is available, coverage gaps can be devastating. Mental health services, reproductive care, and specialty treatments often require additional resources that many plans don't fully cover.
Distance That Blocks Access to Quality Care
Healthcare deserts are real, and they disproportionately affect communities with large Hispanic populations. In rural areas and urban neighborhoods alike, finding a nearby clinic or specialist can mean traveling hours for care. This distance barrier combines with work schedules and family responsibilities to make healthcare practically inaccessible for many women.
When the nearest mammography facility is two hours away, or when you need to take a full day off work to see a specialist, preventive care becomes nearly impossible. These geographic barriers contribute to later diagnoses and poorer health outcomes.
Cultural Misunderstandings in Healthcare Settings
Healthcare works best when there's trust and understanding between patients and providers. Yet many Latina women report feeling misunderstood or judged in medical settings. Cultural differences in how pain is expressed, family involvement in health decisions, or traditional healing practices are sometimes dismissed or misinterpreted by healthcare providers.
These cultural disconnects can lead to misdiagnosis, inappropriate treatment plans, or women feeling so uncomfortable that they avoid care altogether. When your cultural background is seen as an obstacle rather than context, healing becomes much harder.
Discrimination That Hurts Healing
No one should face bias when seeking healthcare, yet studies consistently show that Latina women experience discrimination in medical settings. This might manifest as shorter appointment times, dismissive attitudes toward their concerns, or assumptions about their ability to understand or follow treatment plans.
Research shows that perceived discrimination in healthcare settings leads to delayed care, missed appointments, and worse health outcomes. When you expect to be treated poorly, you're less likely to seek the care you need.
Mental Health Care That Doesn’t Fit
Mental health challenges affect Latina women at significant rates, yet cultural stigma and limited access to appropriate care create additional barriers. Depression, anxiety, and trauma may go untreated when mental health services aren't culturally responsive or when seeking help is seen as a sign of weakness.
The shortage of Spanish-speaking mental health providers means long wait times and limited options for those who do seek care. Without culturally competent mental health services, many women struggle in silence.
Moving Forward Together
These barriers are real, but they're not insurmountable. Change happens when we acknowledge these systemic challenges and work together to address them. Communities are creating innovative solutions: mobile clinics bringing care to underserved areas, community health worker programs providing culturally competent support, and advocacy groups fighting for policy changes.
Healthcare should be a right, not a privilege determined by your zip code, language, or bank account. By understanding these barriers and supporting organizations working to eliminate them, we can help create a healthcare system that truly serves all women.
Learn more: Check out the following resources for support, advocacy, information, and more:
National Latina Institute for Reproductive Justice
Works to advance reproductive justice for Latinas and their families
latinainstitute.org
National Alliance for Hispanic Health
Provides health resources and advocacy for Hispanic communities
healthyamericas.org
UnidosUS
Advocates for Latino civil rights and health equity
unidosus.org
Salud America!
Research and advocacy network for Latino health
salud-america.org
9 Ways to Stand with Black Mothers—and Help Build a Healthier Future

As Black Maternal Health Week draws to a close, we’re called to reflect on what it truly means to stand with Black mothers: to confront systemic inequities with clear-eyed action, while fiercely nurturing the resilience and joy that have always been at the heart of their journeys.
Here are nine ways to turn that reflection into meaningful steps forward:
Advocate for Postpartum Medicaid Expansion
Most states as well as Washington, D.C., offer 12 months of postpartum Medicaid coverage, but Arkansas has yet to adopt this critical support, and Wisconsin limits coverage to 90 days. Closing these gaps could save lives. Forty-three states are also working to make doula care reimbursable through Medicaid—a step toward ensuring every mother has access to compassionate, culturally aligned support during childbirth.
Amplify Black-Led Maternal Health Organizations
Groups like the Black Mamas Matter Alliance and Sisters in Loss are not just organizations—they’re movements. Their community-rooted work—from policy advocacy to grief support—is reshaping systems that have long failed Black mothers. Donate, volunteer, or share their stories. Trust their leadership.
Invest in Black Perinatal Providers
Research shows that Black perinatal professionals—midwives, doulas, and OB-GYNs—deliver care that directly improves outcomes for Black mothers. Yet their representation remains disproportionately low. Advocate for funding training programs and scholarships to grow this essential workforce.
Support Doula Care for All
Doulas act as advocates, confidants, and guides during pregnancy and birth, yet cost barriers leave many Black mothers without this support. Organizations like Ancient Song Doula Services and ROOTT are leading the charge for equitable access. Push for policies that ensure Medicaid and private insurers cover doula services in all states.
Center Postpartum Mental Health
Up to 44% of Black mothers experience postpartum depressive symptoms, but systemic gaps mean many suffer in silence. Programs like the Shades of Blue Project—which offers peer-led support groups and culturally sensitive counseling—are proving that healing happens when care meets compassion. Demand universal mental health screenings and funding for these programs.
Bridge Care Gaps
Telehealth platforms like Maven Clinic connect Black mothers in underserved areas to care teams that understand their lived experiences. These tools are lifelines, offering everything from lactation support to prenatal checkups. Advocate for policies that expand broadband access and telehealth funding so no mother is left behind.
Confront Environmental Injustices
Lead pipes, air pollution, and toxic housing disproportionately harm Black communities—and these environmental risks directly impact maternal health. States like Illinois and Ohio have some of the highest rates of lead exposure. Support clean water initiatives and housing justice campaigns. A mother’s environment should protect her, not put her at risk.
Listen to Black Mothers’ Stories
Too often, Black mothers’ concerns are dismissed or downplayed in medical settings. Platforms created by and for Black women are amplifying their voices, from community-led birth justice collectives to advocacy campaigns. Share these stories, and let them guide policy changes that prioritize dignity and respect.
Address Preterm Birth Disparities
Black women are nearly four times more likely to be hospitalized for uterine fibroids and face preterm birth rates 1.5 times higher than white women. These disparities aren’t inevitable—they’re a result of systemic neglect. Demand increased funding for research and equitable treatment protocols that prioritize Black women’s health.
Where to Learn More:
Black Mamas Matter Alliance: https://blackmamasmatter.org
SisterSong (Reproductive Justice Collective): https://sistersong.net
National Black Midwives Alliance: https://www.blackmidwivesalliance.org
Shades of Blue Project (Mental Health Support): https://www.shadesofblueproject.org
Uschi Keszler: From Olympic Coach to Cancer Research Champion

When Uschi Keszler steps onto the ice, something remarkable happens. Athletes straighten their posture, focus intensifies, and possibilities expand. The same transformative energy now fuels her mission against cancer—turning research dollars into hope for patients worldwide.
Uschi Keszler has built a legacy of excellence, resilience and dedication in both sports and healthcare. The former Olympic athlete and six-time Olympic coach has shaped the careers of figure skating greats including Brian Orser, Elaine Zayak, Elvis Stojko, Claudia Leistner, Tanja Szewczenko and Surya Bonaly. Her story, however, extends well beyond the skating world.
Keszler's journey includes personal health battles, having overcome tuberculosis in her youth and later fighting both breast and uterine cancer. These experiences inspired her to become a devoted advocate for cancer research. In 2007, she founded Pennies in Action, an organization dedicated to raising funds for cutting-edge cancer treatment research.
Her primary focus supports the work of Dr. Brian Czerniecki, whose innovative approach harnesses the body's immune system to fight cancer without the devastating side effects of traditional chemotherapy and radiation.
The same discipline, strategy and relentless pursuit of excellence that Keszler instilled in her athletes now drives her commitment to ensuring Dr. Czerniecki's team receives support for essential clinical trials. She views this effort as a "Gold Medal" win for humanity – a victory that could shift the entire paradigm of cancer treatment.
Keszler envisions both effective treatments and renewed hope for patients seeking alternatives to conventional cancer therapies. Through Pennies in Action, she has helped raise critical funds supporting clinical trials and research, providing hope to patients who may otherwise have limited options.
At The State of Women Institute, we celebrate Uschi Keszler for her contributions to both sports and the fight against cancer. Her ability to apply principles of discipline, resilience and teamwork to medical research advancement is truly inspiring. Through Pennies in Action, her advocacy for groundbreaking cancer therapies, and her determination to achieve nothing less than a "Gold Medal" solution to cancer, Keszler continues to lead the charge against this devastating disease.
Showers of Hope will be held at the Desmond Hotel (Malvern PA) on April 12. For more information, visit https://penniesinaction.org.
Celebrating National Doctors’ Day: Women in Medicine Transform Health Outcomes

Today, we celebrate National Doctors’ Day—and as an organization focused on women’s rights and especially women’s health, we know this isn’t just about gratitude. It’s about recognizing what decades of research confirm: Women doctors are essential to achieving better health outcomes for women. Over the past 50 years, women have surged from 7% of U.S. physicians in 1960 to over 38% today. Progress? Yes. But equality? Not yet. Women doctors still face pay gaps, leadership disparities, and systemic barriers—particularly women of color. Yet study after study shows that when women lead in medicine, care improves for everyone. Today, we honor their contributions and reaffirm why their voices matter.
A Legacy of Breakthroughs, Not Just Firsts—And Room for Improvement
Women have always been healers, but systemic exclusion defined much of medical history. In 1849, Elizabeth Blackwell became the first woman to earn a U.S. medical degree, despite classmates voting to reject her admission. Twenty years later, Dr. Rebecca Lee Crumpler became the first Black woman physician, publishing A Book of Medical Discourses in 1883—a groundbreaking guide to caring for women and children post-slavery. These pioneers didn’t just break rules; they rewrote them.
By the 1970s, activism opened doors for women in medical schools. But progress was uneven. Early 20th-century policies that standardized medical education also shuttered institutions serving marginalized communities, sidelining Black doctors for decades. Today, while women dominate medical school classrooms, they remain underrepresented in leadership: only 22% of full professors and 18% of hospital CEOs are women. The path to parity, it turns out, is paved with both milestones and setbacks.
When Women Lead, Health Outcomes Improve
The evidence is undeniable: women doctors save lives. A 2018 JAMA Internal Medicine study found female heart attack patients treated by women physicians were significantly more likely to survive. Researchers attribute this to women doctors’ adherence to clinical guidelines and collaborative communication styles. Another 2020 study revealed women physicians spend 10% more time with patients—critical for conditions like endometriosis or fibroids, which take an average of 7 years to diagnose.
Dr. Ashish Jha, Dean of Brown’s School of Public Health, put it plainly in The Atlantic: “Patients, especially women, are more likely to share sensitive concerns with female doctors. That trust isn’t incidental—it’s transformative.” Studies show women are 24% more likely to receive preventive care and 20% more likely to adhere to treatment plans when their doctor is a woman.
Today’s Innovators: Bridging Gaps, Saving Lives
Modern women doctors aren’t just filling roles—they’re fixing systems. Pediatrician Dr. Mona Hanna-Attisha leveraged community trust to expose the Flint water crisis, proving lead contamination’s harm to children after officials dismissed parents’ concerns. Immunologist Dr. Kizzmekia Corbett co-developed the Moderna COVID-19 vaccine while advocating for equitable distribution to underserved communities. And Dr. Susan Moore, a Black physician, used her final days in a COVID-19 ICU to document racist neglect in her own care, sparking a national conversation about bias in medicine.
Their work isn’t just about medicine; it’s about justice.
The Future Depends on Equity
Barriers remain stark. A 2021 study found Black scientists receive 55% fewer NIH grants than white peers, limiting research into conditions disproportionately affecting women of color. As Dr. Uché Blackstock writes in her 2024 book Legacy, “We don’t just need more women in medicine—we need systems that value their insights.” Institutions like Meharry Medical College, a historically Black school, are training doctors to serve marginalized communities, proving representation alone isn’t enough. Equity requires funding mentorship, closing pay gaps, and amplifying voices too often unheard.
Women Doctors Are Healthcare’s Foundation
This National Doctors’ Day, we celebrate women physicians not as exceptions, but as proof of what healthcare could be. From Elizabeth Blackwell’s defiant graduation to Dr. Susan Moore’s courageous advocacy, their stories show that women don’t just belong in medicine—they redefine it. Better outcomes for women start with women’s leadership. And as the data shows, that’s not a hope. It’s a fact.
Sources: Association of American Medical Colleges (AAMC), JAMA Internal Medicine, University of Pennsylvania School of Medicine, National Institutes of Health (NIH), The Atlantic, Legacy: A Black Physician Reckons with Racism in Medicine by Dr. Uché Blackstock (2024).